Inverse Biophysical Modeling and Machine Learning in Personalized Oncology
Abstract
This report documents the program and the outcomes of Dagstuhl Seminar 23022 “Inverse Biophysical Modeling and Machine Learning in Personalized Oncology”.
This seminar brought together leading experts in mathematical, computational, and medical imaging sciences with research interests in data science, scientific machine learning, modeling and numerical simulation, optimization, and statistical and deterministic inversion, and image analysis with applications in medical imaging, and, in particular, oncology. A central theme of the seminar was the integration of data-driven methods with model-driven approaches for predictive modeling.
The seminar had several main thrusts including design and analysis of novel mathematical models, recent developments in medical imaging, machine learning in the context data analytics and data-driven model prediction, predictive computational modeling through (statistical) inversion, integration of machine learning with model-based priors and use of these methods to aid decision-making. We discussed these topics through the lens of foundational algorithmic complications and mathematical and computational challenges. The participants explored how advances in the applied sciences (e.g., data analytics, medical imaging, or radiomics) can aid us to tackle challenges in the application domain. We also discussed the significant challenges associated with the validation of the proposed methodology, and a lack of reproducibility due to the absence of standard protocols for validation of data- and model-driven methods by translational research groups.
Keywords and phrases:
Bayesian inverse problems, image segmentation, inverse problems, machine learning, medical image analysis, parallel computing, tumor growth simulation and modelingSeminar:
January 8–13, 2023 – https://www.dagstuhl.de/230222012 ACM Subject Classification:
Applied computing Imaging ; Applied computing Life and medical sciences ; Computing methodologies Machine learning algorithms ; Computing methodologies Machine learning approaches ; Mathematics of computing Mathematical optimization ; Mathematics of computing Mathematical software performance ; Mathematics of computing Numerical analysis ; Mathematics of computing SolversCopyright and License:
1 Executive Summary
Andreas Mang (University of Houston, US)
George Biros (University of Texas at Austin, US)
Björn H. Menze (Universität Zürich, CH)
Miriam Schulte (Universität Stuttgart, DE)
License: ![]() Creative Commons BY 4.0 International license © Andreas Mang, George Biros, Björn H. Menze, and Miriam Schulte
Creative Commons BY 4.0 International license © Andreas Mang, George Biros, Björn H. Menze, and Miriam Schulte
Our Dagstuhl Seminar brought together leading experts in computational and applied mathematics, computer science, biomedical imaging, and medical imaging sciences with research interests in data science, machine learning, modeling, optimization, and statistical and deterministic inversion with applications in medical imaging, and – in particular – oncology. Overall, 22 participants (and 5 remote participants) from various scientific disciplines contributed with scientific presentations about their current and future research efforts in these areas.
The seminar had four main thrusts: (i) machine learning in the context of data analytics and data-driven model prediction, (ii) predictive computational modeling through statistical and deterministic inversion, (iii) integration of machine learning with model-based priors, and (iv) use of these methods to aid decision making. We discussed these topics through the lens of foundational algorithmic complications and mathematical and computational challenges. We also explored how advances in the applied sciences (e.g., data analytics, medical imaging, radiomics, genomics, or experimental design) can aid us to tackle challenges associated with the design of computational and mathematical methods.
In the context of predictive computational modeling and deterministic and statistical inversion, we addressed topics ranging from uncertainty quantification, model choices (multiscale versus macroscopic; model-complexity; multispecies versus single-species), regularization strategies, sensitivity analysis, strategies to address the massive computational costs, challenges in the design of hardware-accelerated computational methods with optimal energy efficiency, and strategies to yield the throughput, robustness, and reliability required in practical applications under given hardware constraints. In the context of machine learning and its integration with predictive modeling and priors, we discussed issues associated with limited reproducibility beyond the training data, robustness against outliers, issues with small-sample size problems, uncertainty quantification for learning from data, and generic strategies to enrich the available data. Lastly, we also explored the availability and use of advanced imaging technologies that can help to (i) provide a better data basis for predictive modeling, (ii) trigger community efforts to enrich available data, and (iii) enable validation and standardize population-based studies. We also discussed reproducibility issues, given that in many cases (medical imaging) data is proprietary, challenges associated with the validation of the proposed methodology, and a lack of reproducibility due to the absence of standard protocols for validation of data- and model-driven methods by translational research groups.
The seminar started with opening remarks by two of the main organizers (Biros and Menze). They reviewed their contributions to the field and gave an overview of the state-of-the-art from their perspective. This opened up the floor for a first discussion on where we are and where we would like to go with our future research. During the first two and a half days different scientists contributed to our seminar with presentations about their recent activities and their view on the state-of-the-art. We did not keep a tightly fixed schedule. This allowed participants to engage and discuss the presented material, shed light on potential future research avenues, identify common areas of interest between participants and research groups, as well as exchange ideas on how to address potential shortcomings of the state-of-the-art methods. Overall, this led to an active exchange about open issues, potential solutions, and current activities among participants of our seminar. The topics discussed during the research presentations include computational and mathematical approaches targeted at aiding clinical treatment (with contributions form, e.g., Brüningk, Fuster Garcia, Hormuth, Menze), the design of new mathematical models of cancer/tumor progression (with contributions from, e.g., Biros, Deutsch, Gomez, Menze, Schulte, Wohlmuth), the design and analysis of methodology for machine learning (with contributions from, e.g., Erhardt, Konukoglu, Pati), inverse problems and optimization (with contributions from, e.g., Biros, Erhardt, Latz, Mang, Schulte), scientific machine learning with applications in medical imaging (with contributions from e.g., Brüningk, Erhardt, Fuster Garcia, Konukoglu, Li, Merhof, Van Leemput), hardware-accelerated computational methods, high performance computing, and computational complexity (with contributions from Biros, Mang, Schulte), the integration of modeling integration of data-driven methods with model-driven approaches for predictive modeling (with contributions from, e.g., Biros, Brüningk, Hormuth, Lorenzo, Menze, Schulte, Wiestler), and advances in medical imaging and medical image analysis (with contributions from, e.g., Li, Lundervold, Merhof, Paech, Pati, Van Leemput, Weidner, Wiestler). Several of these contributions are briefly described in the abstracts included in this report.
As mentioned above, during the discussions after each scientific presentation, we identified several open problems and challenges that we believe should be addressed by the community at large. We briefly list some of the main points raised during these discussions here:
Regarding the integration of computational models with medical imaging, a key challenge is to establish if a model is of use in the clinical context. Many of the available mathematical models are oversimplifications, particularly in the context of modeling cancer progression at a tissue scale. As such, one generic use of these models is to utilize them as “priors” for more classical image analysis tasks such as image segmentation or image registration.
As for generating model-based predictions, a key remaining challenge is how simple or complicated mathematical models need to be, to be of clinical value. While some tasks (e.g., patient classification or tissue characterization) can potentially be helped by simple models, an open question is how complicated models can or have to be to aid clinical decision-making or enable model-based predictions (e.g., if one envisions forecasting the benefit of certain types of clinical intervention in individual patients).
Another key challenge in this context is the scarcity of the available data. Moreover, how do we validate and compare the performance of these approaches and how can we establish good benchmarks to test methods developed by individual research teams? A related open question is, which scale is most suitable to simulate certain aspects of cancer growth/disease progression and/or treatment? Are microscopic rule-based approaches required, or can we utilize coarser, macroscopic models that typically formulate tumor/cancer progression in terms of partial differential equations? Another question is to what extent and if physics-informed methods (i.e., methods based on the simulation of biophysical phenomena) add significant value to clinical diagnosis and treatment planning versus more standard, machine learning-based predictions generated from features derived from imaging data. One key question that was also discussed in this context was how these methods are plagued by model and data uncertainties.
Moreover, we discussed how to integrate modeling with machine learning in the most efficient way. Can we, e.g., use machine learning as a tool to initialize more classical (e.g., variational) methods for inference of model parameters and/or integration of simulation with data? Conversely, can machine learning benefit from an integration of physics-based principles prescribed by biophysical models? Likewise, can machine learning be used as a tool to improve model selection, i.e., can we use it to decide how complex a mathematical model needs to be?
From an imaging perspective, one question that arose was how to combine different types of data (e.g., structural imaging, biomedical markers, radiomics, functional imaging, patient questionnaires) most effectively. In many studies, one typically does not integrate information from multiple sources but relies on specific types of medical data. Would such a more complete integration aid model-based predictions? How does the designed methodology generalize for data acquired at different imaging sites and/or imaging modalities? Another key issue is the scarcity of publicly available (good quality) data and how to address it as a community. One solution presented at the seminar was the use of federated learning.
Lastly, if we envision pushing these methods toward clinical applications, how can we deal with low-performance computing infrastructure at clinical sites? We also discussed clinical scenarios for applying the designed methods and how they could be of use in clinical practice (for example, to plan a therapeutic intervention or post-therapy assessment).
On Wednesday, we engaged participants in scientific discussions during an excursion to an art show at the “Völklinger Hütte”. We concluded this social event with a joint dinner in one of the local restaurants.
The scientific presentations were followed by a brief discussion about selected topics in two working groups to identify immediate goals and further discuss existing challenges. The first group included researchers with a key interest in designing methods to analyze medical (imaging) data and integrate mathematical and computational methods with imaging and medical data. The second group discussed topics associated with the design of mathematical and computational methods for inference, simulation, and optimization. We list the key findings in these two groups and some of the questions that remain to be addressed by the community at large in this report. We concluded our seminar with a plenary discussion about the findings of our working group discussions. This enabled us to identify commonalities toward a more concrete outline of follow-up work after the conclusion of our seminar. As a first concrete goal for the entire group, we agreed that we should start our work with a joint (public) dataset that compiles available medical imaging data for model development and testing. Spearheaded by Gomez and Hormuth, a first list of publicly available data was curated on the Mathematical Oncology webpage: https://mathematical-oncology.org/resources/datasets. Moreover, they have started to collect information for relevant conferences and workshops of interest for the community at large (https://mathematical-oncology.org/conferences).
2 Table of Contents
3 Overview of Talks
3.1 Harnessing machine learning and mechanistic modelling for personalized radiotherapy of pediatric diffuse midline glioma
Sarah Brüningk (ETH Zürich – Basel, CH)
License: ![]() Creative Commons BY 4.0 International license © Sarah Brüningk
Creative Commons BY 4.0 International license © Sarah Brüningk
Joint work of: Sarah Brüningk, Catherine Jutzeler, Javad Nazarian, Karsten Borgwardt, Sabine Mueller
Pediatric diffuse midline glioma is a rare, yet fatal disease, with currently no curative treatment. Owing to the delicate location of these tumors, treatment options and surgical interventions are greatly limited. Radiotherapy (RT) is one of the few life-prolonging treatments, but its therapeutic efficacy varies between individuals. Currently, it is impossible to predict RT benefit a priori and there is a great unmet clinical need to improve patient stratification and survival.
The overarching aim of this project is to build a treatment decision support platform facilitating personalized RT optimization based on non-invasive magnetic resonance imaging. To this end, we develop an analytical pipeline bridging mechanistic modelling and data-driven machine learning to refine patient stratification, discover imaging biomarkers, and inform RT scheduling and dosing by an individualized radiosensitivity score (RSS).
Imaging and clinical data from 250 patients centralized from different international institutions are at the centre of this analysis. Image classification will be based on a scalable combination of local and global image features reflecting the biological hallmarks of DMGs. The challenge of limited, multi-domain data is addressed via the model architecture together with transfer learning from adult glioblastoma and data augmentation. We employ interpretability analysis to identify imaging biomarkers driving classification, and use regression analysis to infer a RSS. An ordinary differential equation model of longitudinal tumor growth under RT is fitted to follow-up patient data. Based on the fitted model parameters and the RSS, alternative RT strategies can then be simulated and the gain in time to progression of an in silico trial comparing conventional and personalized RT will be quantified. At this point we are in the early phase of the study and have centalized patient data from the University of Californa, San Francisco, from The DMG Centre Zurich, and from patients treated as part of clinical trials within the Pacific Pediatric Neuro-Oncology Consortium (PNOC).
This study investigates personalized RT for a group of pediatric patients for which treatment individualization is inevitable. The treatment decision support tool and the identified imaging biomarkers should be translatable to clinical practice, while our in silico trial may motivate clinical evaluation to provide validation of our predictions. By focussing on imaging data and available, cost effective RT, our approach is feasible in treatment facilities worldwide with clear application of digital pediatric health. Relevant references are [1, 2].
Acknowledgements
This project is funded by the Botnar Research Centre for Child Health as part of their postdoctoral excellence programme under #PEP-2021-1008. The ETH Career Seed grant 2021-HS-329 supported the centralization of the data sets.
References
- [1] Kuijs, M., Jutzeler, C. R., Rieck, B., and Brüningk, S. C. (2021). Interpretability aware model training to improve robustness against out-of-distribution Magnetic Resonance Images in Alzheimer’s disease classification. arXiv. https://doi.org/10.48550/arXiv.2111.08701
- [2] Brüningk, S. C., Peacock, J., Whelan, C. J., Brady-Nicholls, R., Yu, H.-H. M., Sahebjam, S., and Enderling, H. (2021). Intermittent radiotherapy as alternative treatment for recurrent high grade glioma: a modeling study based on longitudinal tumor measurements. Scientific Reports, 11(1). https://doi.org/10.1038/s41598-021-99507-2
3.2 Mechanisms of cancer invasion and progression: insights from cellular automaton models
Andreas Deutsch (TU Dresden, DE)
License: ![]() Creative Commons BY 4.0 International license © Andreas Deutsch
Creative Commons BY 4.0 International license © Andreas Deutsch
Tumour invasion and progression may be viewed as collective phenomena emerging from the interplay of biological cells with their environment. Cell-based mathematical models in which cells are regarded as separate discrete entities can be used to decipher the rules of interaction. Here, we focus on the dynamics of glioma and breast cancer. We introduce lattice-gas cellular automaton models [1, 5] to analyse the role of phenotypic plasticity in cancer invasion, define spatial and non-spatial Moran processes to shed light on the size of the tumour originating niche, and adopt Markov chain models to investigate the origin of genetic heterogeneity in glioblastoma [2, 3, 4].
References
- [1] A. Deutsch and S. Dormann, Cellular automaton modeling of biological pattern formation: characterization, applications, and analysis, Birkhauser, Boston, 2018.
- [2] T. Buder, A. Deutsch, B. Klink and A. Voss-Böhme, Patterns of tumor progression predict small and tissue-specific tumor-originating niches, Front. Oncol., 8, 668, 2019.
- [3] Anne Dirkse, Anna Golebiewska, Thomas Buder, Petr V. Nazarov, Arnaud Muller, Suresh Poovathingal, Nicolaas H. C. Brons, Sonia Leite, Nicolas Sauvageot, Dzjemma Sarkisjan, Mathieu Seyfrid, Sabrina Fritah, Daniel Stieber, Alessandro Michelucci, Frank Hertel, Christel Herold-Mende, Francisco Azuaje, Alexander Skupin, Rolf Bjerkvig, Andreas Deutsch, Anja Voss-Böhme and Simone P. Niclou, Stem cell-associated heterogeneity in Glioblastoma results from intrinsic tumor plasticity shaped by the microenvironment, Nature Commun., 10, 1, 1787, 2019.
- [4] Olga Ilina, Pavlo G. Gritsenko, Simon Syga, Jürgen Lippoldt, Caterina A. M. La Porta, Oleksandr Chepizhko, Steffen Grosser, Manon Vullings, Gert-Jan Bakker, Jörn Starruß, Peter Bult, Stefano Zapperi, Josef A. Käs, Andreas Deutsch and Peter Friedl, Cell–cell adhesion and 3D matrix confinement determine jamming transitions in breast cancer invasion, Nature Cell Biol., 1103–1115, 2020.
- [5] A. Deutsch, J. M. Nava-Sedeño, S. Syga, H. Hatzikirou, BIO-LGCA: a cellular automaton modelling class for analysing collective cell migration, PLOS Comp. Biol., 17, 6, e1009066, 2021.
3.3 Machine Learning meets Inverse Problems: Bilevel Learning
Matthias J. Ehrhardt (University of Bath, GB)
License: ![]() Creative Commons BY 4.0 International license © Matthias J. Ehrhardt
Creative Commons BY 4.0 International license © Matthias J. Ehrhardt
Joint work of: Matthias J. Ehrhardt, Lindon Roberts, Ferdia Sherry, Martin Benning, Juan Carlos de los Reyes, Martin J.Graves, Georg Maierhofer, GuyWilliams, Carola-Bibiane Schönlieb
Inverse problems are omnipresent in any imaging related field and is as such a backbone in oncology, too. Here we focussed on the connections of machine learning to the particular inverse problem of image reconstruction but many concepts generalise to other inverse problems such as estimating parameters in PDEs. Solving inverse problems can be approached via variational regularization techniques which are dominant in the field of inverse problems in general. A drawback of these techniques is that they are dependent on a number of parameters which have to be set by the user. This issue can be approached by machine learning where we estimate these parameters from data. This is known as “Bilevel Learning” and has been successfully applied to many tasks, some as small-dimensional as learning a regularization parameter, others as high-dimensional as learning a sampling pattern in MRI. While mathematically appealing this strategy leads to a nested optimization problem which is computationally difficult to handle. We discussed several applications of bilevel learning for imaging [2, 1] as well as new computational approaches [1, 3].
References
- [1] Ehrhardt, M. J., and Roberts, L. (2021).Inexact Derivative-Free Optimization for Bilevel Learning. Journal of Mathematical Imaging and Vision, 63(5), 580–600. https://doi.org/10.1007/s10851-021-01020-8
- [2] Sherry, F., Benning, M., de los Reyes, J. C., Graves, M. J., Maierhofer, G., Williams, G., Schönlieb, C.-B., and Ehrhardt, M. J. (2020). Learning the Sampling Pattern for MRI. IEEE Transactions on Medical Imaging, 39(12), 4310–4321.
- [3] Ehrhardt, M. J., and Roberts, L. (2023). Analyzing Inexact Hypergradients for Bilevel Learning. http://arxiv.org/abs/2301.04764
3.4 Computational Radiology & Artificial Intelligence in Cancer
Elies Fuster Garcia (Technical University of Valencia, ES)
License: ![]() Creative Commons BY 4.0 International license © Elies Fuster Garcia
Creative Commons BY 4.0 International license © Elies Fuster Garcia
Joint work of: Atle Bjornerud, Kyrre E. Emblem, Siri Fløgstad Svensson, Elies Fuster Garcia, Juan M. García-Gómez, F. Javier Gil-Terrón, Qinghui Liu, Carles Lopez-Mateu, Donatas Sederevičius
Recent advances in medical imaging, coupled with the analysis capabilities offered by artificial intelligence, have led to significant progress in personalized oncology. Advanced MRI sequences in neuroimaging are now able to provide critical biophysical parameters for the study of tumor growth, response to therapies, and clinical decision-making. Furthermore, the integration of multi-parametric information, which would be otherwise infeasible, is now made possible through artificial intelligence. This presentation will introduce the collaborative efforts between the Biomedical Data Science Lab (Universitat Politècnica de València, UPV) and the MRI research and technology (Oslo University Hospital, OUH) to combine these two disciplines and make a real impact on clinical practice, particularly on high-grade glial tumors.
The OUH is improving its MRI protocol for neuro-oncology studies by incorporating advanced MRI sequences, such as Vessel Caliber MRI, Vessel Architectural Imaging, and MR Elastography. These sequences offer valuable information at the voxel level, such as vessel caliber size and density [1], vessel type dominance and microvascular efficiency [2], and tissue biomechanics by stiffness and viscosity [3, 8]. This enables researchers to gather a wider range of information on the brain’s blood vessels and tissue, providing a more comprehensive understanding of neuro-oncology.
To integrate all of the information gathered through advanced MRI sequences, processing pipelines and multi-parametric artificial intelligence models are being developed. The collaboration between the Oslo University Hospital (OUH) and the Universitat Politècnica de València (UPV) has led to the creation of AI systems that can accurately segment regions of interest [4], identify functional habitats [5], and analyze longitudinal series and growth dynamics [6], among others. An example of such a system is the publicly available ONCOhabitats platform developed by the UPV, which studies vascular heterogeneity in patients with high-grade glial tumors [7].
The success of these AI technologies in clinical practice depends on their integration into a relevant environment at the moment of decision-making. To achieve this, OUH’s models and associated pipelines are being integrated into a computation framework connected with the hospital PACS through the TrackGrowth, Chronos, and Progress research projects (see Acknowledgements). This setup allows for the direct evaluation of AI-based solutions in PACS by deploying hospital-approved software in the hospital interface.
Acknowledgements
We gratefully acknowledge support from the European Union’s Horizon 2020 Programme: ERC Grant [758657-ImPRESS], Research and Innovation Grant [668039-FORCE], Marie Skłodowska-Curie grant [844646-GLIOHAB]; South-Eastern Norway Regional Health Authority [2017073, 2013069, 2021057]; The Research Council of Norway Grant [261984, 325971, 325971]; the National Institutes of Health R21 grant [EB030757]; the German Research Foundation [SCHR 1542/1-1]; Grant PID2021-127110OA-I00 (PROGRESS) funded by MCIN/AEI/ 10.13039/501100011033 and by ERDF A way of making Europe; Grant PID2019-104978RB-I00/AEI/10.13039/501100011033 (ALBATROSS) funded by MCIN/AEI/ 10.13039/501100011033.
References
- [1] Emblem, K. E. et al. Vessel caliber–a potential MRI biomarker of tumour response in clinical trials. Nat. Rev. Clin. Oncol. 11, (2014).
- [2] Emblem, K. E. et al. Vessel architectural imaging identifies cancer patient responders to anti-angiogenic therapy. Nat. Med. 19, 1178–1183 (2013).
- [3] Fløgstad Svensson, S. et al. Decreased tissue stiffness in glioblastoma by MR elastography is associated with increased cerebral blood flow. Eur. J. Radiol. 147, 110136 (2022).
- [4] Juan-Albarracín, J., Fuster-Garcia, E., Manjon, J. V., Robles, M., Aparici, F., Martí-Bonmatí, L., and Garcia-Gomez, J. M. Automated glioblastoma segmentation based on a multiparametric structured unsupervised classification. PLoS ONE 10, (2015).
- [5] Álvarez-Torres, M. D. M. et al. Robust association between vascular habitats and patient prognosis in glioblastoma: An international multicenter study. J. Magn. Reson. Imaging JMRI (2019) https://doi.org/10.1002/jmri.26958.
- [6] Fuster-Garcia, E. et al. Quantification of Tissue Compression Identifies High-Grade Glioma Patients with Reduced Survival. Cancers 14, 1725 (2022).
- [7] Juan-Albarracín, J., Fuster-Garcia, E., García-Ferrando, G. A. and García-Gómez, J. M. ONCOhabitats: A system for glioblastoma heterogeneity assessment through MRI. Int. J. Med. Inf. 128, 53–61 (2019).
- [8] Siri Fløgstad Svensson, Kyrre Eeg Emblem, and Elies Fuster-Garcia. (2021). MR Elastography, perfusion and diffusion data in 9 patients with glioblastoma and 17 healthy subjects [Data set]. Zenodo. https://doi.org/10.5281/zenodo.4926005
3.5 An image-driven computational modeling approach to forecast radiotherapy response in gliomas
David Hormuth (University of Texas at Austin, US)
License: ![]() Creative Commons BY 4.0 International license © David Hormuth
Creative Commons BY 4.0 International license © David Hormuth
Joint work of: David A. Hormuth II, Karine A. Al Feghali, Andrew M. Elliott, Thomas E. Yankeelov, Caroline Chung
Radiotherapy (RT) is a foundational component of clinical management for high-grade glioma (HGG) used to target residual and infiltrative disease following surgical resection. Variability in patient response to radiotherapy can depend on the tumor’s underlying sensitivity to treatment as well as the ability to accurately target the biologically relevant malignant tissue. To improve patient outcomes, RT treatment plans could be adapted for individual patients to target tumor sub-regions demonstrating treatment resilience and higher aggressive potential. Towards this goal, we developed a family of biologically-based mathematical models of HGG growth and response, which are initialized and calibrated using patient-specific multi-parametric magnetic resonance imaging (mpMRI) data [1, 2]. Our family of models is built upon a 3D, two-species model of enhancing and non-enhancing tumor that describes tumor cell proliferation, diffusion, and treatment response. Unique to our approach is the use of mpMRI collected weekly during RT which reports on both tumor extent and cellularity dynamics. Using patient imaging data collected before treatment onset and weekly up to mid-treatment, we identified patient-specific tumor growth and response parameters via a non-linear least squares optimization. These patient-specific model parameters were then used to forecast tumor growth and response dynamics at the remaining weekly imaging visits during RT. In an initial cohort of 13 patients, we observed that our computational framework was able to predict total tumor cell count with a Pearson correlation coefficient of 0.95 and concordance correlation coefficient of 0.91 at 1-month post-RT. Likewise, the forecasted total tumor volume agreed spatially with the observed tumor volume with Dice similarity coefficients greater than 0.73. At the individual voxel-level, the forecasted distribution of tumor growth was able to predict areas of significant increases or decreases in tumor cell with an accuracy, specificity, and sensitivity greater than 0.76. The results of this initial study demonstrates the ability for image-driven modeling to predict HGG response to RT that with further development may enable anticipatory adaption of RT.
Acknowledgements
NCI R01CA235800, U24CA226110, U01CA174706, CPRIT RR160005 and CPRIT RP220225. Caroline Chung is supported by the Andrew Sabin Family Foundation Fellowship, MD Anderson Cancer Center Institutional Research Grant and CCSG Radiation Oncology and Cancer Imaging Program, and the Marnie Rose Foundation. T.E.Y. is a CPRIT Scholar in Cancer Research.
References
- [1] Hormuth II DA, Feghali KA Al, Elliott AM, Yankeelov T, Chung C. Image-based personalization of computational models for predicting response of high-grade glioma to chemoradiation. Scientific Reports. 2021;11:1-14. https://doi.org/10.1038/s41598-021-87887-4
- [2] Hormuth DA, Farhat M, Christenson C, et al. Opportunities for improving brain cancer treatment outcomes through imaging-based mathematical modeling of the delivery of radiotherapy and immunotherapy. Advanced Drug Delivery Reviews. 2022;187:114367. https://doi.org/10.1016/j.addr.2022.114367
3.6 On the well-posedness of Bayesian inverse problems
Jonas Latz (Heriot-Watt University – Edinburgh, GB)
License: ![]() Creative Commons BY 4.0 International license © Jonas Latz
Creative Commons BY 4.0 International license © Jonas Latz
Main reference: Jonas Latz: “On the Well-posedness of Bayesian Inverse Problems”, SIAM/ASA J. Uncertain. Quantification, Vol. 8(1), pp. 451–482, 2020.
Mathematical models that are used in science and engineering often need to be calibrated with respect to observational data. In the context of tumour modelling, for instance, image data can be used to estimate chemotaxis, consumption, and proliferation of a tumour [1]. Such parameter estimation problems are often referred to as “inverse problems”. Due to observational noise and complexity of models, inverse problems are usually difficult to solve and also ill-posed: a well-posed problem on the opposite is one, that has a solution, the solution is unique, and the solution depends continuously on the data. Well-posedness is important. Without existence, the problem has no solution and is, thus, not solvable. Uniqueness is required to prevent ambiguity between different solutions. The continuity assumption is a stability condition: the data is noisy, thus, we should hope that the influence of the noise on the parameter estimate is restricted in a certain sense.
The Bayesian approach to inverse problems gives a way to turn an ill-posed inverse problem into a well-posed problem. Here, we consider the calibration problem to be a statistical problem and model noise and unknown parameter as random variables. Through conditioning we are then able to incorporate the information from the data into the parameter. The conditioning can be achieved through Bayes’ formula.
As shown in [2], the resulting “Bayesian inverse problem” will be well-posed under very, very mild assumptions, allowing for parameter estimation in blackbox models and, e.g., with respect to data-driven prior models.
References
- [1] Christian Kahle, Kei Fong Lam, Jonas Latz and Elisabeth Ullmann. Bayesian parameter identification in Cahn-Hilliard models for biological growth. SIAM/ASA Journal on Uncertainty Quantification 7(2): 526-552, 2019.
- [2] Jonas Latz. On the Well-posedness of Bayesian inverse problems. SIAM/ASA Journal on Uncertainty Quantification 8(1): 451–482, 2020.
3.7 Intelligent Neuroimaging for Precision Neuro-oncology
Chao Li (University of Cambridge, GB)
License: ![]() Creative Commons BY 4.0 International license © Chao Li
Creative Commons BY 4.0 International license © Chao Li
Brain tumour comprises a spectrum of malignant and benign entities. The complex pathophysiology of brain tumours poses challenges to effective clinical decision-making and treatment for patients. Multi-modal neuroimaging provides a non-invasive technique for probing brain tumours [5, 3, 13]. Based on neuroimaging, artificial intelligence (AI) offers an automated solution to optimise patient management, promising to accelerate precision neuro-oncology. Typically, the clinical applications of AI include tools for automatic diagnostics and guiding precise treatment. Together, these AI models promise to improve the overall efficiency of healthcare. Through engaging clinical domain knowledge, AI models can be tailored to the critical challenges in neuro-oncology, which could further advance our understanding of brain tumours and accelerate individualised and precise therapeutics.
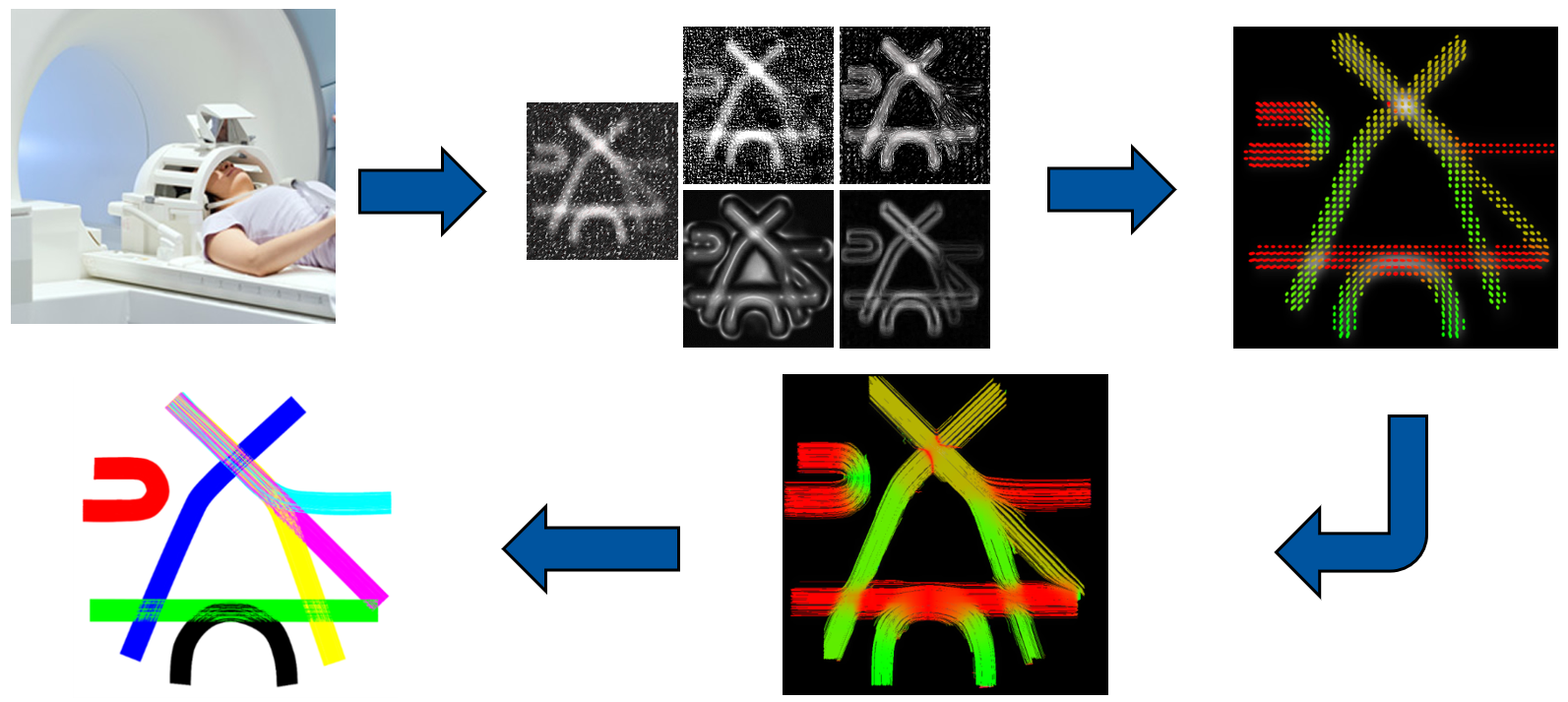
Glioma is the most common malignant brain tumour in adults, characterised by remarkable heterogeneity and extensive invasion. To characterize tumour heterogeneity based on imaging, we designed novel radiological features to characterize tumour morphology and spatial heterogeneity [12]. Combined with machine learning methods, these features show robust performance in subtyping patients across diverse tissues and imaging modalities. The identified patient sub-groups show distinct molecular characteristics and prognostics. Advanced MRI techniques, e.g., perfusion and diffusion MRIs [4, 6], provide sensitive information for characterising tumour invasion over contrast-enhanced MRI. However, advanced MRI are typically in low resolution, which hinders full training labels for developing supervised models. To mitigate this challenge, we develop weakly supervised deep learning models that can identify the tumour invasion outside of contrast enhancement [2]. Further, glioma is considered a systematic disease, as it frequently spreads along white matter tracts into the whole brain. To characterize the tumour invasion globally, we developed an iterative tract-based spatial statistics method to quantify the structural connectivity of the brain and measure tract integrity in brain tumour patients [11]. Through comparing patients to healthy controls, we identified regional disrupted connectome in glioblastoma patients, which shows significance in predicting patient survival and indicating treatment targets [10]. Following this study, we introduced brain connectome into the AI model to better characterise glioma. Specifcially, we developed a multi-modal learning model, which leverages three encoders to extract features of focal tumour image, tumour geometrics and global brain network in predicting the isocitrate dehydrogenase (IDH) mutation, achieving higher performance over other state-of-the-art models [9].
In translating AI models into real-world practice, we need to tackle the challenges from heterogeneous clinical datasets, e.g., missing scans, and low image resolution. Therefore, we develop AI approaches to enhance image quality and standardisation [7, 1, 8]. For a trustworthy AI solution, we develop biophysics-informed deep learning models to enhance model explainability and generalisability. With these AI prototypes developed, we test the models in the real-world clinical setting, by connecting model development with the clinical system to obtain clinical and biological validations. We develop multi-centre imaging trials to validate the efficacy of imaging tools, where MR images are processed using reproducible and transparent pipelines. In the next step, we will test the imaging tools at scale through connections to large population data. Our vision is to transform the healthcare of brain tumour patients using image-based AI models.
Acknowledgements
Supported by Guarantors of Brain.
References
- [1] Jiang, L., Mao, Y., Chen, X., Wang, X., Li, C.: Cola-diff: Conditional latent diffusion model for multi-modal mri synthesis. arXiv preprint arXiv:2303.14081 (2023).
- [2] Li, C., Huang, W., Chen, X., Wei, Y., Price, S.J., Schönlieb, C.B.: Expectation-maximization regularized deep learning for weakly supervised tumor segmentation for glioblastoma. arXiv preprint arXiv:2101.08757 (2021).
- [3] Li, C., Wang, S., Serra, A., Torheim, T., Yan, J.L., Boonzaier, N.R., Huang, Y., Matys, T., McLean, M.A., Markowetz, F., et al.: Multi-parametric and multi-regional histogram analysis of MRI: Modality integration reveals imaging phenotypes of glioblastoma. European Radiology, 29, 4718–4729 (2019).
- [4] Li, C., Wang, S., Yan, J.L., Piper, R.J., Liu, H., Torheim, T., Kim, H., Zou, J., Boonzaier, N.R., Sinha, R., et al.: Intratumoral heterogeneity of glioblastoma infiltration revealed by joint histogram analysis of diffusion tensor imaging. Neurosurgery 85(4), 524–534 (2019).
- [5] Li, C., Wang, S., Yan, J.L., Torheim, T., Boonzaier, N.R., Sinha, R., Matys, T., Markowetz, F., Price, S.J.: Characterizing tumor invasiveness of glioblastoma using multiparametric magnetic resonance imaging. Journal of Neurosurgery 132(5), 1465–1472 (2019)
- [6] Li, C., Yan, J.L., Torheim, T., McLean, M.A., Boonzaier, N.R., Zou, J., Huang, Y., Yuan, J., van Dijken, B.R., Matys, T., et al.: Low perfusion compartments in glioblastoma quantified by advanced magnetic resonance imaging and correlated with patient survival. Radiotherapy and Oncology 134, 17–24 (2019).
- [7] Liu, P., Li, C., Schönlieb, C.B.: Ganredl: Medical image enhancement using a generative adversarial network with real-order derivative induced loss functions. In: Medical Image Computing and Computer Assisted Intervention–MICCAI 2019: 22nd International Conference, Shenzhen, China, October 13–17, 2019, Proceedings, Part III 22. pp. 110–117. Springer (2019).
- [8] Mao, Y., Jiang, L., Chen, X., Li, C.: Disc-diff: Disentangled conditional diffusion model for multi-contrast mri super-resolution. arXiv preprint arXiv:2303.13933 (2023).
- [9] Wei, Y., Chen, X., Zhu, L., Zhang, L., Schönlieb, C.B., Price, S., Li, C.: Multi-modal learning for predicting the genotype of glioma. IEEE Transactions on Medical Imaging (2023).
- [10] Wei, Y., Li, C., Cui, Z., Mayrand, R.C., Zou, J., Wong, A. L. K. C., Sinha, R., Matys, T., Schönlieb, C.B., Price, S.J.: Structural connectome quantifies tumour invasion and predicts survival in glioblastoma patients. Brain 146(4), 1714–1727 (2023).
- [11] Wei, Y., Li, C., Price, S.J.: Quantifying structural connectivity in brain tumor patients. In: Medical Image Computing and Computer Assisted Intervention–MICCAI 2021: 24th International Conference, Strasbourg, France, September 27–October 1, 2021, Proceedings, Part VII 24. pp. 519–529. Springer (2021)
- [12] Wu, J., Li, C., Gensheimer, M., Padda, S., Kato, F., Shirato, H., Wei, Y., Schönlieb, C.B., Price, S.J., Jaffray, D., et al.: Radiological tumour classification across imaging modality and histology. Nature Machine Intelligence 3(9), 787–798 (2021).
- [13] Yan, J.L., Li, C., Boonzaier, N.R., Fountain, D.M., Larkin, T.J., Matys, T., van der Hoorn, A., Price, S.J.: Multimodal MRI characteristics of the glioblastoma infiltration beyond contrast enhancement. Therapeutic advances in neurological disorders 12, 1756286419844664 (2019)
3.8 Personalized computational forecasting of prostate cancer growth during active surveillance
Guillermo Lorenzo (University of Pavia, IT & UT Austin, US)
License: ![]() Creative Commons BY 4.0 International license © Guillermo Lorenzo
Creative Commons BY 4.0 International license © Guillermo Lorenzo
Joint work of: Guillermo Lorenzo, Jon S. Heiselman, Michael A. Liss, Michael I. Miga, Hector Gomez, Thomas E. Yankeelov, Thomas J. Hughes, Alessandro Reali
Active surveillance (AS) is a feasible management option for low to intermediate-risk prostate cancer (PCa), which represents almost 70% of newly-diagnosed cases. During AS, patients have their tumor monitored via multiparametric magnetic resonance imaging (mpMRI), serum prostate-specific antigen (PSA), and biopsies [1]. If any of these data reveal tumor progression towards an increased clinical risk, the patient is prescribed a curative treatment. However, clinical decision-making in AS is usually guided by population-based protocols that do not account for the unique, heterogenous nature of each patient’s tumor. This limitation complicates the personalization of monitoring plans and the early detection of tumor progression, which constitute two unresolved problems in AS. To address these issues, we propose to forecast PCa growth using personalized simulations of an mpMRI-informed mechanistic model solved over the 3D anatomy of the patient’s prostate [1, 2, 3]. We describe PCa growth via the dynamics of tumor cell density with a diffusion operator, representing tumor cell mobility, and a logistic reaction term, which accounts for tumor cell net proliferation [1, 2]. Model calibration and validation rely on assessing the mismatch between model predictions of the tumor cell density map with respect to corresponding mpMRI-based estimates [2]. Our preliminary results on a cohort of seven patients show a median concordance correlation coefficient (CCC) and Dice score (DSC) of 0.55 and 0.82, respectively, for the spatial fit of tumor cell density during model calibration using two mpMRI datasets. Then, model validation at the date of a third mpMRI scan resulted in median CCC and DSC of 0.33 and 0.76, respectively. Thus, while further improvement and testing in larger cohorts are required, we believe that our results are promising for the potential use of our methods to personalize AS protocols and predict tumor progression.
References
- [1] G. Lorenzo, J.S. Heiselman, M.A. Liss, M.I. Miga, H. Gomez, T.E. Yankeelov, T.J.R. Hughes, and A. Reali. Patient-specific forecasting of prostate cancer growth during active surveillance using an imaging-informed mechanistic model, Cancer Research, 82(12 Supp): 5064, 2022.
- [2] G. Lorenzo, D.A. Hormuth II, A.M. Jarrett, E.A.B.F. Lima, S. Subramanian, G. Biros, J.T. Oden, T.J.R. Hughes, and T.E. Yankeelov. Quantitative in vivo imaging to enable tumor forecasting and treatment optimization. In: Cancer, Complexity, Computation. Eds.: Igor Balaz and Andrew Adamatzky, Springer, pp. 55-97, 2023.
- [3] G. Lorenzo, M.A. Scott, K. Tew, T.J.R. Hughes, Y.J. Zhang, L. Liu, G. Vilanova, and H. Gomez. Tissue-scale, personalized modeling and simulation of prostate cancer growth, Proceedings of the National Academy of Sciences of the United States of America, 113(48): E7663-E7671, 2016.
3.9 Scalable Algorithms for Diffeomorphic Image Registration
Andreas Mang (University of Houston, US)
License: ![]() Creative Commons BY 4.0 International license © Andreas Mang
Creative Commons BY 4.0 International license © Andreas Mang
Joint work of: Andreas Mang, George Biros, Malte Brunn, Naveen Himthani, Miriam Schulte
We present a framework for diffeomorphic image registration termed CLAIRE [1, 6]. This algorithm is an integral part of some of our efforts to develop algorithms for the analysis of brain tumor imaging data [4, 5, 7, 8, 9]. Diffeomorphic image registration is a non-linear, ill-posed inverse problem that poses significant mathematical and computational challenges. Generally speaking, we seek a -diffeomorphism , that establishes a point-wise spatial correspondence between two views (images) of the same scene. In our work, we consider a variational formulation governed by hyperbolic transport equations.
Our contributions are new algorithms and dedicated computational kernels to reduce the runtime. We study the performance of our solver in terms of rate of convergence, registration accuracy, and time-to-solution. We demonstrate that we can solve problems for clinically relevant data of sizes ( voxels; 50 million unknowns) in under 5 seconds (see table below). Our formulation and numerical algorithms are described in [6, 10, 11, 13]. Our parallel CPU implementation is discussed in [6, 12]. Our parallel GPU implementation is presented in [2, 3]. The integration of our registration algorithm with models of tumor progression is presented in [4, 5, 7, 8, 9]. We overview the computational performance of our framework for diffeomorphic image registration for an image of size in the table below. Compared to our CPU implementation we observe a speedup between 28 and 71 depending on the GPU and implementation (CLAIRE: standard implementation; CLAIRE∗: additional intermediate variables kept in memory). We report from left to right the version of CLAIRE, the hardware CLAIRE is executed on, the memory use, the mismatch between the data after registration, the runtime in seconds and the speedup. We can see that the GPU implementation is significantly faster than our GPU implementation without sacrificing accuracy.
| version | hardware | mem | mis | runtime | speedup |
| CLAIRE | 24 core x86 | 2.9e-2 | 1.5e2 | 1 | |
| P100 | 4.6GB | 2.6e-2 | 5.2e0 | 28 | |
| V100 | 4.6GB | 2.6e-2 | 4.2e0 | 36 | |
| RTX3080 | 5.0GB | 2.6e-2 | 3.2e0 | 47 | |
| CLAIRE∗ | P100 | 8.1GB | 3.6e-2 | 2.9e0 | 52 |
| 4V100 | 2.6GB | 3.6e-2 | 2.1e0 | 71 | |
| RTX3080 | 8.5GB | 3.6e-2 | 2.3e0 | 65 |
Acknowledgments
This work was partly supported by the National Science Foundation under the awards DMS-1854853, DMS-2012825, and DMS-2145845. Any opinions, findings, and conclusions or recommendations expressed herein are those of the authors and do not necessarily reflect the views of NSF.
References
- [1] M. Brunn, N. Himthani, G. Biros, M. Mehl and A. Mang. CLAIRE: Constrained Large Deformation Diffeomorphic Image Registration on Parallel Computing Architectures. The Journal of Open Source Software, 6(61), 3038, 2021.
- [2] M. Brunn, N. Himthani, G. Biros, M. Mehl and A. Mang. Fast GPU 3D diffeomorphic image registration. Journal of Parallel and Distributed Computing, 149:149–162, 2021.
- [3] M. Brunn, N. Himthani, G. Biros, M. Mehl and A. Mang. Multi-node multi-GPU diffeomorphic image registration for large-scale imaging problems. Proc ACM/IEEE Conference on Supercomputing, pp. 523–539, 2020.
- [4] A. Mang, S. Bakas, S. Subramanian, G. Biros and C. Davatzikos. Integrated biophysical modeling and image analysis: Application to neuro-oncology. Annual Review of Biomedical Engineering, 22:309–341, 2020.
- [5] K. Scheufele, S. Subramanian, A. Mang, G. Biros and M. Mehl. Image-driven biophysical tumor growth model calibration. SIAM Journal on Scientific Computing, 42(3):B549–B580, 2020.
- [6] A. Mang, A. Gholami, C. Davatzikos and G. Biros. CLAIRE: A distributed-memory solver for constrained large deformation diffeomorphic image registration. SIAM Journal on Scientific Computing, 41(5):C548–C584, 2019.
- [7] K. Scheufele, A. Mang, A. Gholami, C. Davatzikos, G. Biros and M. Mehl. Coupling brain-tumor biophysical models and diffeomorphic image registration. Computer Methods in Applied Mechanics and Engineering, 237:533–567, 2019.
- [8] A. Mang, A. Gholami, C. Davatzikos and G. Biros. PDE-constrained optimization in medical image analysis. Optimization and Engineering, 19(3):765–812, 2018.
- [9] A. Gholami, A. Mang, K. Scheufele, C. Davatzikos, M. Mehl and G. Biros. A framework for scalable biophysics-based image analysis. Proc ACM/IEEE Conference on Supercomputing, 19:1–19:13, 2017.
- [10] A. Mang and G. Biros. A semi-Lagrangian two-level preconditioned Newton–Krylov solver for constrained diffeomorphic image registration. SIAM Journal on Scientific Computing, 39(6):B1064–B1101, 2017.
- [11] A. Mang and L. Ruthotto. A Lagrangian Gauss–Newton–Krylov solver for intensity- and mass-preserving diffeomorphic image registration. SIAM Journal on Scientific Computing, 39(5):B860–B885, 2017.
- [12] A. Mang, A. Gholami and G. Biros. Distributed-memory large-deformation diffeomorphic 3D image registration. Proc ACM/IEEE Conference on Supercomputing, pp. 842–853, 2016.
- [13] A. Mang and G. Biros. Constrained -regularization schemes for diffeomorphic image registration. SIAM Journal on Imaging Sciences, 9(3):1154–1194, 2016.
- [14] A. Mang and G. Biros. An inexact Newton–Krylov algorithm for constrained diffeomorphic image registration. SIAM Journal on Imaging Sciences, 8(2):1030–1069, 2015.
3.10 Deep-Learning based Analysis of Diffusion MRI Data
Dorit Merhof (Universität Regensburg, DE)
License: ![]() Creative Commons BY 4.0 International license © Dorit Merhof
Creative Commons BY 4.0 International license © Dorit Merhof
Joint work of: Dorit Merhof, Leon Weninger, Simon Koppers, Chuh-Hyoun Na, Kerstin Jütten, Hans Clusmann, Veren Mainz, Seigfried Gauggel, Ferdinand Binkofski, Martin Wiesmann, Christoph Haarburger, Sandro Romanzetti, Julia Ebert, Kathrin Reetz, Mushawar Ahmad, Lu Bloy
Artificial Intelligence approaches, and especially recent Deep Learning techniques, have shown to outperform conventional image processing algorithms in many medical image analysis scenarios.
This presentation will present Deep Learning approaches for Diffusion MRI Data for (1) diffusion signal augmentation [1], (2) free water correction [6, 2, 4] and (3) signal harmonization [5, 6, 7].
Finally, limitations of neuronal networks as well as current challenges and trends in Deep Learning will be discussed.

References
- [1] Simon Koppers, Christoph Haarburger and Dorit Merhof: Diffusion MRI Signal Augmentation – From Single Shell to Multi Shell with Deep Learning. In: MICCAI Workshop on Computational Diffusion MRI (CDMRI), 2016.
- [2] Leon Weninger, Simon Koppers, Chuh-Hyoun Na, Kerstin Juetten and Dorit Merhof: Free-Water Correction in Diffusion MRI: A Reliable and Robust Learning Approach. In: MICCAI Workshop on Computational Diffusion MRI (CDMRI), 2019.
- [3] Leon Weninger, Chuh-Hyoun Na, Kerstin Jütten and Dorit Merhof: Analyzing the effects of free water modeling by deep learning on diffusion MRI structural connectivity estimates in glioma patients. In: PLOS ONE 15 (9), 2020.
- [4] Kerstin Jütten, Leon Weninger, Verena Mainz, Siegfried Gauggel, Ferdinand Binkofski, Martin Wiesmann, Dorit Merhof, Hans Clusmann and Chuh-Hyoun Na: Dissociation of structural and functional connectomic coherence in glioma patients. In: Scientific Reports 11 (16790), 2021.
- [5] Simon Koppers, Luke Bloy, Jeffrey I. Berman, Chantal M.W. Tax, J. Christopher Edgar and Dorit Merhof: Spherical Harmonic Residual Network for Diffusion Signal Harmonization. In: MICCAI Workshop on Computational Diffusion MRI (CDMRI), 2018.
- [6] Leon Weninger, Sandro Romanzetti, Julia Ebert, Kathrin Reetz and Dorit Merhof: Harmonization of diffusion MRI data obtained with multiple head coils using hybrid CNNs. In: ECCV AIMIA Workshop, 2022.
- [7] Leon Weninger, Mushawar Ahmad and Dorit Merhof: From supervised to unsupervised harmonization of diffusion MRI acquisitions. In: IEEE International Symposium on Biomedical Imaging (ISBI), 2022.
3.11 Federated Learning and Reproducibility in Healthcare
Sarthak Pati (University of Pennsylvania, US)
License: ![]() Creative Commons BY 4.0 International license © Sarthak Pati
Creative Commons BY 4.0 International license © Sarthak Pati
Joint work of: Sarthak Pati, Spyridon Bakas
Real-world applicability of artificial intelligence (AI) in the clinical setting [39, 40, 41] is hampered by the i) lack of available diverse (training and validation) data affecting the robustness and generalizability of AI models towards unseen/unknown population groups, and ii) limitations on defining reproducible computational pipelines for local hardware resources at clinical sites.
The current paradigm towards sufficiently large and diverse data for training and validating AI models is via centralization of data from multiple institutions [29, 30, 32, 33, 31, 17, 6, 49, 50, 45, 46, 47, 48, 51]. However, this paradigm faces limitations when it comes to scale due to various legal, regulatory, cultural, and ownership concerns [8, 9]. Federated Learning (FL) offers an alternative paradigm to train robust AI models and a potential solution to the data sharing hurdles, as demonstrated in multiple simulated [8, 9, 2, 43] and real-world studies [1]. Furthermore, beyond training robust AI models, the evaluation of their effectiveness and durability over time on real-world patient data from large and diverse population demographics poses another challenge towards their clinical translation. Federated evaluation (FE) studies through persistent data registries and streamlined workflows may provide a solution on such performance evaluations, obviating the need of data sharing. Together, federated learning and evaluation form complementary mechanisms to generate meaningful clinical impact by enabling access to data silos in a way that is compatible with regulations and cultural concerns.
There have been numerous community-driven efforts to provide either common definitions towards results’ reproducibility [13, 14, 16, 29, 30, 32, 33, 31, 17, 49, 50, 45, 46, 47, 48, 51], or common benchmarking environments (i.e., challenges) for fair AI model evaluation [15]. Although a substantial number of closed-source and commercial solutions achieve clinical reproducibility [42], having widely available, community-driven, and well-documented open-source projects [18, 19, 20, 21, 22, 23, 34, 7] that focus on the reproducibility of research, while being driven by the clinical stakeholders would be critical towards ensuring that cutting edge scientific breakthroughs make it for clinical validation sooner. This further allows computational scientists to explore their methodological interests while allowing clinical partners to deploy these methods in an easy manner in their existing hardware infrastructure.
Our collaborative group has collectively produced open-source publicly-available software solutions to address this space. Starting with the largest real-world FL study to-date (the Federated Tumor Segmentation (FeTS) initiative)555www.fets.ai, which also describes the largest reported study on the rare cancer of glioblastoma, involving data of 6,314 patients from 71 institutions across 6 continents [1]. The tool used by the FeTS Initiative has been open-sourced as “The FeTS Tool” [4], which provides an end-to-end point solution for studies related to brain tumor boundary detection/segmentation. This solution includes all the required computational steps, starting from data curation, anonymization, brain extraction (also known as skull-stripping [35, 34]), to pre-processing, generation of baseline automated annotations leveraging methods considered state of the art [53, 54, 55], an interface to manually refine these automated annotations and sign off ground truth labels [18, 19, 20], as well as to allow a user to either train their AI model or join an existing FL study. Moreover, the FL component of the FeTS tool is enabled by the Open Federated Learning (OpenFL) library [11, 10], which is designed for general-purpose FL and being agnostic to use-case and framework. Further to the FeTS initiative, OpenFL has facilitated studies on the i) effect of cosmic radiation on astronauts by the Frontier Development Lab (FDL) of the National Aeronautics and Space Administration (NASA), and ii) prediction of respiratory distress syndrome and death for COVID-19 patients by the 11 sites of the Montefiore Health System in New York.
Building upon the collaborative network of the FeTS initiative, we further conducted the first-ever computational challenge in FL, which happened in conjunction with the International Conference on Medical Image Computing and Computer Assisted Intervention (MICCAI) 2021 and 2022 [5], and followed the principle of clinical trials [52]. The focus of the FeTS challenge was two-fold: i) the development of aggregation methods for FL, and ii) the federated evaluation of brain tumor segmentation algorithms in-the-wild, by circulating AI models on unseen data from multiple sites of the FeTS initiative collaborative network. The FeTS challenge was orchestrated by MedPerf [24], in which the challenge organizers initiated the design of the study, the collaborating sites registered information about their datasets, and the AI models of the challenge participants were described as independent experiments evaluated against these datasets. Finally, towards broader clinical workflows, we developed the Generally Nuanced Deep Learning Framework (GaNDLF) [12], which enables users to design and manage AI algorithms for multiple tasks and various data/organ/modality types, such as segmentation on brain tumor MRI [2, 1], breast mammograms [37, 36] & dynamic contrast enhanced MRI [6], as well as classification on histology whole slide images [3], RGB images [38], & breast mammograms [43]. The wide applicability and obtained results showcase the generalizability of GaNDLF. Additionally, GaNDLF offers automated post-training optimization of AI models [56, 44], allowing their execution/inference on consumer-grade computers without requiring specialized hardware, such as deep learning acceleration cards.
In conclusion, there is a need to i) assess the generalizability of AI models by capturing ample patient demographics, ii) address bias and inequities in AI, especially those related to underserved/underrepresented patient populations, and iii) on the continuous monitoring of AI models requiring further developments in automated quality control, monitoring of drift & bias, and model calibration. Towards fulfilling these goals, the open federated ecosystem consisting of GaNDLF [12], OpenFL [11], and MedPerf [24] provide a holistic end-to-end open-sourced federated learning and evaluation solution that supports multiple data types, and that be easily used by both experienced and novice researchers.
Acknowledgements
Research reported in this publication was partly supported by the National Cancer Institute (NCI) of the National Institutes of Health (NIH) under award number U01CA242871. The content of this publication is solely the responsibility of the authors and does not represent the official views of the NIH or any other funding body.
References
- [1] Pati, S., Baid, U., Edwards, B., Sheller, M., Wang, S., Reina, G., Foley, P., Gruzdev, A., Karkada, D., Davatzikos, C. et al. Federated Learning Enables Big Data for Rare Cancer Boundary Detection.Nature Communications. 13 (2022)
- [2] Baid, U., Pati, S., Thakur, S., Edwards, B., Sheller, M., Martin, J. & Bakas, S. The Federated Tumor Segmentation (FeTS) Initiative: The First Real-World Large-Scale Data-Private Collaboration Focusing On Neuro-Oncology. Neuro-Oncology. 23 pp. 135-135 (2021)
- [3] Baid, U., Pati, S., Kurc, T., Gupta, R., Bremer, E., Abousamra, S., Thakur, S., Saltz, J. and Bakas, S. Federated learning for the classification of tumor infiltrating lymphocytes. ArXiv Preprint ArXiv:2203.16622. (2022)
- [4] Pati, S., Baid, U., Edwards, B., Sheller, M., Foley, P., Reina, G., Thakur, S., Sako, C., Bilello, M., Davatzikos, C. et al. The federated tumor segmentation (FeTS) tool: an open-source solution to further solid tumor research. Physics In Medicine & Biology. 67, 204002 (2022)
- [5] Pati, S., Baid, U., Zenk, M., Edwards, B., Sheller, M., Reina, G., Foley, P., Gruzdev, A., Martin, J., Albarqouni, S. et al. The Federated Tumor Segmentation (FeTS) Challenge. ArXiv Preprint ArXiv:2105.05874. (2021)
- [6] Chitalia, R., Pati, S., Bhalerao, M., Thakur, S., Jahani, N., Belenky, V., McDonald, E., Gibbs, J., Newitt, D., Hylton, N. et al. Expert tumor annotations and radiomics for locally advanced breast cancer in DCE-MRI for ACRIN 6657/I-SPY1.Scientific Data. 9, 440 (2022).
- [7] Bounias, D., Singh, A., Bakas, S., Pati, S., Rathore, S., Akbari, H., Bilello, M., Greenberger, B., Lombardo, J., Chitalia, R. et al. Interactive machine learning-based multi-label segmentation of solid tumors and organs. Applied Sciences. 11, 7488 (2021)
- [8] Sheller, M., Reina, G., Edwards, B., Martin, J. and Bakas, S. Multi-institutional deep learning modeling without sharing patient data: A feasibility study on brain tumor segmentation. International MICCAI Brainlesion Workshop. pp. 92-104 (2018)
- [9] Sheller, M., Edwards, B., Reina, G., Martin, J., Pati, S., Kotrotsou, A., Milchenko, M., Xu, W., Marcus, D., Colen, R. et al. Federated learning in medicine: Facilitating multi-institutional collaborations without sharing patient data. Scientific Reports. 10, 1-12 (2020)
- [10] Reina, G., Gruzdev, A., Foley, P., Perepelkina, O., Sharma, M., Davidyuk, I., Trushkin, I., Radionov, M., Mokrov, A., Agapov, D. et al. OpenFL: An open-source framework for Federated Learning. ArXiv Preprint ArXiv:2105.06413. (2021)
- [11] Foley, P., Sheller, M., Edwards, B., Pati, S., Riviera, W., Sharma, M., Moorthy, P., Wang, S., Martin, J., Mirhaji, P. et al. OpenFL: the open federated learning library. Physics In Medicine & Biology. 67, 214001 (2022)
- [12] Pati, S., Thakur, S., Bhalerao, M., Baid, U., Grenko, C., Edwards, B., Sheller, M., Agraz, J., Baheti, B., Bashyam, V. et al. Gandlf: A generally nuanced deep learning framework for scalable end-to-end clinical workflows in medical imaging. ArXiv Preprint ArXiv:2103.01006. (2021)
- [13] Zwanenburg, A., Vallières, M., Abdalah, M., Aerts, H., Andrearczyk, V., Apte, A., Ashrafinia, S., Bakas, S., Beukinga, R., Boellaard, R. et al. The image biomarker standardization initiative: standardized quantitative radiomics for high-throughput image-based phenotyping. Radiology. 295, 328-338 (2020)
- [14] McNitt-Gray, M., Napel, S., Jaggi, A., Mattonen, S., Hadjiiski, L., Muzi, M., Goldgof, D., Balagurunathan, Y., Pierce, L., Kinahan, P. et al. Standardization in quantitative imaging: A multicenter comparison of radiomic features from different software packages on digital reference objects and patient data sets. Tomography. 6, 118-128 (2020)
- [15] Eisenmann, M., Reinke, A., Weru, V., Tizabi, M., Isensee, F., Adler, T., Godau, P., Cheplygina, V., Kozubek, M., Ali, S. et al. Biomedical image analysis competitions: The state of current participation practice. ArXiv Preprint ArXiv:2212.08568. (2022)
- [16] Pati, S., Verma, R., Akbari, H., Bilello, M., Hill, V., Sako, C., Correa, R., Beig, N., Venet, L., Thakur, S. et al. Reproducibility analysis of multi-institutional paired expert annotations and radiomic features of the Ivy Glioblastoma Atlas Project (Ivy GAP) dataset. Medical Physics. 47, 6039-6052 (2020)
- [17] Borovec, J., Kybic, J., Arganda-Carreras, I., Sorokin, D., Bueno, G., Khvostikov, A., Bakas, S., Eric, I., Chang, C., Heldmann, S. et al. ANHIR: automatic non-rigid histological image registration challenge. IEEE Transactions On Medical Imaging. 39, 3042-3052 (2020)
- [18] Davatzikos, C., Rathore, S., Bakas, S., Pati, S., Bergman, M., Kalarot, R., Sridharan, P., Gastounioti, A., Jahani, N., Cohen, E. et al. Cancer imaging phenomics toolkit: Quantitative imaging analytics for precision diagnostics and predictive modeling of clinical outcome. Journal Of Medical Imaging. 5, 011018 (2018)
- [19] Pati, S., Singh, A., Rathore, S., Gastounioti, A., Bergman, M., Ngo, P., Ha, S., Bounias, D., Minock, J., Murphy, G. et al. The Cancer Imaging Phenomics Toolkit (CaPTk): Technical Overview. International MICCAI Brainlesion Workshop. pp. 380-394 (2019)
- [20] Rathore, S., Bakas, S., Pati, S., Akbari, H., Kalarot, R., Sridharan, P., Rozycki, M., Bergman, M., Tunc, B., Verma, R. et al. Brain cancer imaging phenomics toolkit (brain-CaPTk): an interactive platform for quantitative analysis of glioblastoma. International MICCAI Brainlesion Workshop. pp. 133-145 (2017)
- [21] Fathi Kazerooni, A., Akbari, H., Shukla, G., Badve, C., Rudie, J., Sako, C., Rathore, S., Bakas, S., Pati, S., Singh, A. et al. Cancer imaging phenomics via CaPTk: Multi-institutional prediction of progression-free survival and pattern of recurrence in glioblastoma. JCO Clinical Cancer Informatics. 4 pp. 234-244 (2020)
- [22] Wolf, I., Vetter, M., Wegner, I., Nolden, M., Bottger, T., Hastenteufel, M., Schobinger, M., Kunert, T. and Meinzer, H. The medical imaging interaction toolkit (MITK): a toolkit facilitating the creation of interactive software by extending VTK and ITK. Medical Imaging 2004: Visualization, Image-Guided Procedures, And Display. 5367 pp. 16-27 (2004)
- [23] Kikinis, R., Pieper, S. and Vosburgh, K. 3D Slicer: a platform for subject-specific image analysis, visualization, and clinical support. Intraoperative Imaging And Image-guided Therapy. pp. 277-289 (2014)
- [24] Karargyris, A., Umeton, R., Sheller, M., Aristizabal, A., George, J., Bala, S., Beutel, D., Bittorf, V., Chaudhari, A., Chowdhury, A. et al. MedPerf: Open Benchmarking Platform for Medical Artificial Intelligence using Federated Evaluation. ArXiv Preprint ArXiv:2110.01406. (2021)
- [25] Beam, A., Manrai, A. and Ghassemi, M. Challenges to the reproducibility of machine learning models in health care. Jama. 323, 305-306 (2020)
- [26] Belbasis, L. and Panagiotou, O. Reproducibility of prediction models in health services research. BMC Research Notes. 15, 1-5 (2022)
- [27] Benjamin Haibe-Kains, George Alexandru Adam, Ahmed Hosny, Farnoosh Khodakarami, Massive Analysis Quality Control Society Board of Directors, Levi Waldron, Bo Wang, Chris McIntosh, Anna Goldenberg, Anshul Kundaje, Casey S. Greene, Tamara Broderick, Michael M. Hoffman, Jeffrey T. Leek, Keegan Korthauer, Wolfgang Huber, Alvis Brazma, Joelle Pineau, Robert Tibshirani, Trevor Hastie, John P. A. Ioannidis, John Quackenbush and Hugo J. W. L. Aerts. Transparency and reproducibility in artificial intelligence. Nature. 586, E14-E16 (2020)
- [28] Carter, R., Attia, Z., Lopez-Jimenez, F. and Friedman, P. Pragmatic considerations for fostering reproducible research in artificial intelligence. NPJ Digital Medicine. 2, 1-3 (2019)
- [29] Menze, B., Jakab, A., Bauer, S., Kalpathy-Cramer, J., Farahani, K., Kirby, J., Burren, Y., Porz, N., Slotboom, J., Wiest, R. et al. The multimodal brain tumor image segmentation benchmark (BRATS). IEEE Transactions On Medical Imaging. 34, 1993-2024 (2014)
- [30] Bakas, S., Reyes, M., Jakab, A., Bauer, S., Rempfler, M., Crimi, A., Shinohara, R., Berger, C., Ha, S., Rozycki, M. et al. Identifying the best machine learning algorithms for brain tumor segmentation, progression assessment, and overall survival prediction in the BRATS challenge. ArXiv Preprint ArXiv:1811.02629. (2018)
- [31] Baid, U., Ghodasara, S., Mohan, S., Bilello, M., Calabrese, E., Colak, E., Farahani, K., Kalpathy-Cramer, J., Kitamura, F., Pati, S. et al. The RSNA-ASNR-MICCAI BraTS 2021 benchmark on brain tumor segmentation and radiogenomic classification. ArXiv Preprint ArXiv:2107.02314. (2021)
- [32] Bakas, S., Akbari, H., Sotiras, A., Bilello, M., Rozycki, M., Kirby, J., Freymann, J., Farahani, K. and Davatzikos, C. Segmentation labels and radiomic features for the pre-operative scans of the TCGA-LGG collection. The Cancer Imaging Archive. 286 (2017)
- [33] Bakas, S., Akbari, H., Sotiras, A., Bilello, M., Rozycki, M., Kirby, J., Freymann, J., Farahani, K. and Davatzikos, C. Segmentation labels and radiomic features for the pre-operative scans of the TCGA-GBM collection. The Cancer Imaging Archive. 286 (2017)
- [34] Thakur, S., Doshi, J., Pati, S., Rathore, S., Sako, C., Bilello, M., Ha, S., Shukla, G., Flanders, A., Kotrotsou, A. et al. Brain extraction on MRI scans in presence of diffuse glioma: Multi-institutional performance evaluation of deep learning methods and robust modality-agnostic training. NeuroImage. 220 pp. 117081 (2020)
- [35] Thakur, S., Doshi, J., Pati, S., Ha, S., Sako, C., Talbar, S., Kulkarni, U., Davatzikos, C., Erus, G. and Bakas, S. Skull-stripping of glioblastoma MRI scans using 3D deep learning. Brainlesion: Glioma, Multiple Sclerosis, Stroke And Traumatic Brain Injuries: 5th International Workshop, BrainLes 2019, Held In Conjunction With MICCAI 2019, Shenzhen, China, October 17, 2019, Revised Selected Papers, Part I. pp. 57-68 (2020)
- [36] Ahluwalia, V., Mankowski, W., Pati, S., Bakas, S., Brooks, A., Vachon, C., Conant, E., Gastounioti, A. and Kontos, D. Artificial-intelligence-driven volumetric breast density estimation with digital breast tomosynthesis in a racially diverse screening cohort.. (American Society of Clinical Oncology,2022)
- [37] Ahluwalia, V., Mankowski, W., Pati, S., Bakas, S., Brooks, A., Vachon, C., Conant, E., Gastounioti, A. and Kontos, D. Deep-learning-enabled volumetric breast density estimation with digital breast tomosynthesis. Cancer Research. 82, 1929-1929 (2022)
- [38] Güley, O., Pati, S. and Bakas, S. Classification of Infection and Ischemia in Diabetic Foot Ulcers Using VGG Architectures. Diabetic Foot Ulcers Grand Challenge. pp. 76-89 (2021)
- [39] Giger, M. Machine learning in medical imaging. Journal Of The American College Of Radiology. 15, 512-520 (2018)
- [40] Kelly, C., Karthikesalingam, A., Suleyman, M., Corrado, G. and King, D. Key challenges for delivering clinical impact with artificial intelligence. BMC Medicine. 17 pp. 1-9 (2019)
- [41] Ashton, J., Young, A., Johnson, M. and Beattie, R. Using machine learning to impact on long-term clinical care: principles, challenges, and practicalities. Pediatric Research. pp. 1-10 (2022)
- [42] Rexilius, J., Spindler, W., Jomier, J., König, M., Hahn, H., Link, F. and Peitgen, H. A framework for algorithm evaluation and clinical application prototyping using ITK. Insight Journal—MICCAI Open-Source Workshop. (2005)
- [43] Katti, K., Muthukrishnan, R., Heyler, A., Pati, S., Alahari, A., Sanborn, M., Conant, E., Scott, C., Winham, S., Vachon, C. et al. MammoDL: Mammographic Breast Density Estimation using Federated Learning. ArXiv Preprint ArXiv:2206.05575. (2022)
- [44] Thakur, S., Pati, S., Panchumarthy, R., Karkada, D., Wu, J., Kurtaev, D., Sako, C., Shah, P. and Bakas, S. Optimization of Deep Learning Based Brain Extraction in MRI for Low Resource Environments. International MICCAI Brainlesion Workshop. pp. 151-167 (2022)
- [45] Baheti, B., Waldmannstetter, D., Chakrabarty, S., Akbari, H., Bilello, M., Wiestler, B., Schwarting, J., Calabrese, E., Rudie, J., Abidi, S. et al. The brain tumor sequence registration challenge: establishing correspondence between pre-operative and follow-up MRI scans of diffuse glioma patients. ArXiv Preprint ArXiv:2112.06979. (2021)
- [46] Simpson, A., Antonelli, M., Bakas, S., Bilello, M., Farahani, K., Van Ginneken, B., Kopp-Schneider, A., Landman, B., Litjens, G., Menze, B. et al. A large annotated medical image dataset for the development and evaluation of segmentation algorithms. ArXiv Preprint ArXiv:1902.09063. (2019)
- [47] Bilic, P., Christ, P., Li, H., Vorontsov, E., Ben-Cohen, A., Kaissis, G., Szeskin, A., Jacobs, C., Mamani, G., Chartrand, G. et al. The liver tumor segmentation benchmark (lits). Medical Image Analysis. 84 pp. 102680 (2023)
- [48] Antonelli, M., Reinke, A., Bakas, S., Farahani, K., Kopp-Schneider, A., Landman, B., Litjens, G., Menze, B., Ronneberger, O., Summers, R. et al. The medical segmentation decathlon. Nature Communications. 13, 4128 (2022)
- [49] Davatzikos, C., Barnholtz-Sloan, J., Bakas, S., Colen, R., Mahajan, A., Quintero, C., Capellades Font, J., Puig, J., Jain, R., Sloan, A. et al. AI-based prognostic imaging biomarkers for precision neuro-oncology: the ReSPOND consortium. Neuro-oncology. 22, 886-888 (2020)
- [50] Bakas, S., Ormond, D., Alfaro-Munoz, K., Smits, M., Cooper, L., Verhaak, R. and Poisson, L. iGLASS: imaging integration into the Glioma Longitudinal Analysis Consortium. Neuro-oncology. 22, 1545-1546 (2020)
- [51] Dorent, R., Kujawa, A., Ivory, M., Bakas, S., Rieke, N., Joutard, S., Glocker, B., Cardoso, J., Modat, M., Batmanghelich, K. et al. CrossMoDA 2021 challenge: Benchmark of cross-modality domain adaptation techniques for vestibular schwannoma and cochlea segmentation. Medical Image Analysis. 83 pp. 102628 (2023)
- [52] Larson, D., Harvey, H., Rubin, D., Irani, N., Justin, R. and Langlotz, C. Regulatory frameworks for development and evaluation of artificial intelligence–based diagnostic imaging algorithms: summary and recommendations. Journal Of The American College Of Radiology. 18, 413-424 (2021)
- [53] Kamnitsas, K., Ledig, C., Newcombe, V., Simpson, J., Kane, A., Menon, D., Rueckert, D. and Glocker, B. Efficient multi-scale 3D CNN with fully connected CRF for accurate brain lesion segmentation. Medical Image Analysis. 36 pp. 61-78 (2017)
- [54] McKinley, R., Meier, R. and Wiest, R. Ensembles of densely-connected CNNs with label-uncertainty for brain tumor segmentation. International MICCAI Brainlesion Workshop. pp. 456-465 (2018)
- [55] Isensee, F., Jaeger, P., Kohl, S., Petersen, J. and Maier-Hein, K. nnU-Net: a self-configuring method for deep learning-based biomedical image segmentation. Nature Methods. 18, 203-211 (2021)
- [56] Baheti, B., Thakur, S., Pati, S., Karkada, D., Panchumarthy, R., Wu, J., Mohan, S., Nasrallah, M., Shah, P. and Bakas, S. Optimization of artificial intelligence algorithms for low-resource/clinical environments: Focus on clinically-relevant glioma region delineation. Neuro-Oncology. 24 pp. 167-167 (2022)
3.12 Coupling Brain Tumor Models and Image Registration
Miriam Schulte (Universität Stuttgart, DE)
License: ![]() Creative Commons BY 4.0 International license © Miriam Schulte
Creative Commons BY 4.0 International license © Miriam Schulte
Joint work of: Miriam Schulte, George Biros, Malte Brunn, Amir Gholami, Andreas Mang, Klaudius Scheufele, Shashank Subramanian
We present computational coupling of inverse tumor simulation and diffeomorphic image registration that allows to achieve two tasks that can be relevant for clinicians: (i) registration of a healthy statistical atlas brain to a patient brain with tumor in order to transfer labels and brain region boundaries; (ii) identification of tumor growth parameters such as diffusion and reaction rates or initial tumor. For both tasks, we have to solve a combined inverse problem involving image registration and the tumor model to ’move’ from an atlas image to a patient images with a tumor. We present various ways to achieve this by combining separate registration and tumor solvers in [1, 2]. More details on the single components are presented in [3] for the tumor growth inversion and in [4] for image registration. Both software components show very good scalability on high performance computing hardware such that we can solve problems at resolution in a couple of minutes.
References
- [1] Klaudius Scheufele. Coupling Schemes and Inexact Newton for Multi-Physics and Coupled Optimization Problems, Doctoral Thesis, University of Stuttgart, Germany, 2019, https://doi.org/10.18419/opus-10396.
- [2] Klaudius Scheufele, Andreas Mang, Amir Gholami, Christos Davatzikos, George Biros and Miriam Mehl. Coupling brain-tumor biophysical models and diffeomorphic image registration. Computer Methods in Applied Mechanics and Engineering, Volume 347, pages 533-567, 2019, https://doi.org/10.1016/j.cma.2018.12.008.
- [3] Shashank Subramanian, Klaudius Scheufele, Miriam Mehl and George Biros. Where did the tumor start? An inverse solver with sparse localization for tumor growth models. IOP Publishing Ltd, Inverse Problems, Volume 36, Number 4, 2020, https://doi.org/10.1088/1361-6420/ab649c.
- [4] Malte Brunn, Naveen Himthani, George Biros, Miriam Mehl and Andreas Mang. Multi-Node Multi-GPU Diffeomorphic Image Registration for Large-Scale Imaging Problems. SC20: International Conference for High Performance Computing, Networking, Storage and Analysis, Atlanta, GA, USA, 2020, pp. 1-17, https://doi.org/10.1109/SC41405.2020.00042.
- [5] Gerasimos Chourdakis, Kyle Davis, Benjamin Rodenberg, Miriam Schulte, Frédéric Simonis, Benjamin Uekermann, Georg Abrams, Hans-Joachim Bungartz, Lucia Cheung Yau, Ishaan Desai, Konrad Eder, Richard Hertrich, Florian Lindner, Alexander Rusch, Dmytro Sashko, David Schneider, Amin Totounferoush, Dominik Volland, Peter Vollmer and Oguz Ziya Koseomur. preCICE v2: A sustainable and user-friendly coupling library. Open Res Europe 2022, https://doi.org/10.12688/openreseurope.14445.2.
3.13 Generative Models for Generalizable and Interpretable Analysis of Brain Tumor Images
Koen Van Leemput (Martinos Center – Charlestown, US)
License: ![]() Creative Commons BY 4.0 International license © Koen Van Leemput
Creative Commons BY 4.0 International license © Koen Van Leemput
In my talk I will discuss the use of generative models for generalizable and interpretable analysis of brain tumor images. Specifically, I will highlight the fundamental differences that exist between analyzing tightly-standardized images in well-controlled group studies, vs. analyzing images acquired “in the wild”, i.e., as part of the clinical treatment of brain diseases. I will present our work on generative models that can naturally extrapolate beyond the narrow characteristics of manually labeled training data, and how these techniques are implemented within the well-known open-source software suite FreeSurfer. Specific attention will be paid to modeling lesions (such as white matter lesions or brain tumors) within whole-brain segmentation settings, and to leveraging the temporal consistency between follow-up scans in longitudinal data. Time permitting, I will also touch on the need for interpretable image prediction models, where the generative aspect encodes the causal effect of disease on brain shape. Such models are much easier to interpret and explain to clinicians than the “black box” discriminative methods that are often used for predicting diagnoses or disease scores from images.
3.14 A Clinical and Biological Validation Study of a Tumor Growth Model
Benedikt Wiestler (TU München – Klinikum rechts der Isar, DE)
License: ![]() Creative Commons BY 4.0 International license © Benedikt Wiestler
Creative Commons BY 4.0 International license © Benedikt Wiestler
Joint work of: Marie-Christin Metz, Ivan Ezhov, Lucas Zimmer, Jan C. Peeken, Josef A. Buchner, Jana Lipkova, Florian Kofler, Diana Waldmannstetter, Claire Delbridge, Christian Diehl, Denise Bernhardt, Friederike Schmidt-Graf, Jens Gempt, Stephanie E. Combs, Claus Zimmer, Bjoern Menze, Benedikt Wiestler
The diffuse growth pattern of glioblastoma is one of the main challenges for improving patient survival. Computational tumor growth modeling has emerged as a promising tool to infer tumor cell distribution and thereby guide personalized therapy.
In [1], we performed clinical and biological validation of a novel, deep learning – based growth model [2], aiming to close the gap between the experimental state and clinical implementation. In more detail, we wanted to investigate how well this Fisher-Kolmogorov model correlates with (i) tumor biology, (ii) survival and – perhaps most importantly – (iii) location of tumor recurrence.
To answer these questions, we included a total of three data sets into our study. For (i) and (ii), we analysed 124 patients from The Cancer Genome Archive network and 397 patients from the UCSF glioma MRI data set for correlations between clinical data, genetic pathway activation maps (generated with PARADIGM; TCGA only), and infiltration (Dw) as well as proliferation () parameters stemming from a Fisher-Kolmogorov growth model adjusted to the patients’ preoperative images [2]. To address (iii), we correlated later tumor recurrence in an in-house data set with 30 glioblastoma patients with radiotherapy plans and growth model-derived tumor cell distribution.
Interestingly, we observed a significant correlation between 11 signaling pathways that are associated with proliferation, and the estimated proliferation parameter . The parameter ratio Dw/ (p<0.05 in TCGA) as well as the simulated tumor volume (p<0.05 in both TCGA and UCSF) were significantly inversely correlated with overall survival in Cox survival modeling. Depending on the cutoff value for tumor cell density, we observed a significant improvement of recurrence coverage without significantly increased radiation volume utilizing model-derived target volumes instead of standard radiation plans (example shown in figure 2).
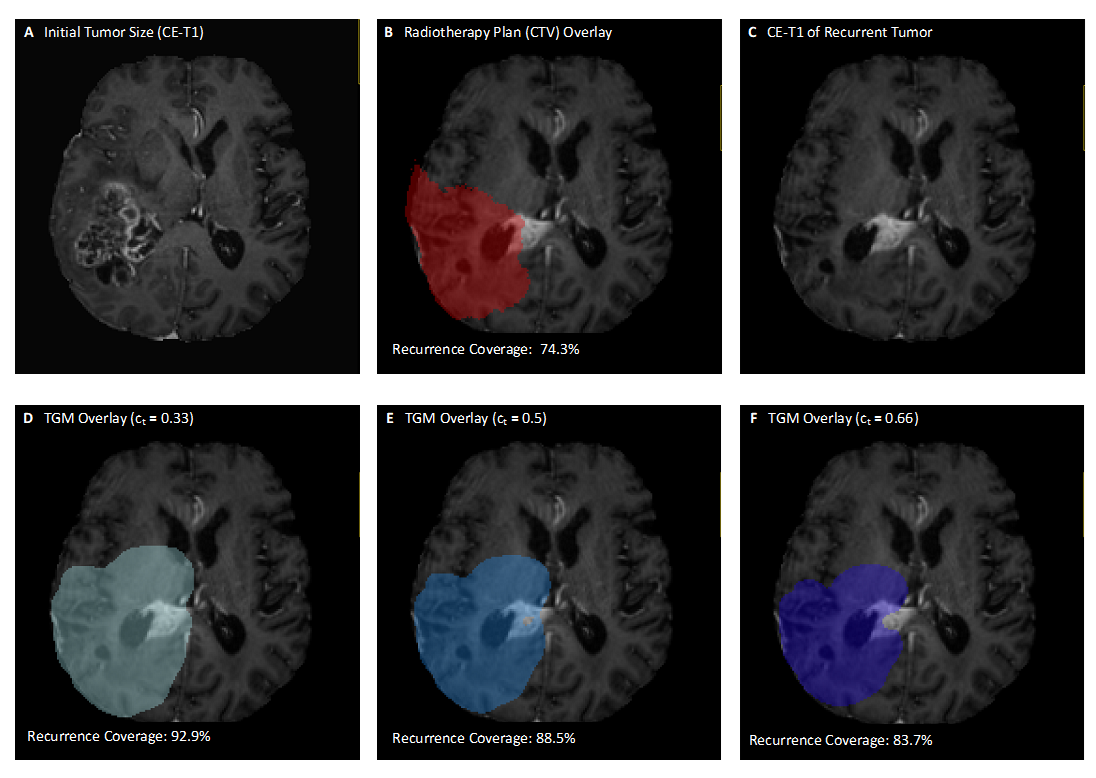
Identifying a significant correlation between computed growth parameters, and clinical and biological data, we highlight the potential of tumor growth modeling for individualized therapy of glioblastoma. This holds promise to improve accuracy of personalized radiation planning in the near future. Future research directions include more complex growth models (e.g., including necrosis or mass effect), including imaging information for model calibration, and ultimately also going from global to local modeling, explicitly incorporating tumor heterogeneity.
References
- [1] Metz M, Ezhov I, Zimmer L, Peeken JC, Buchner JA, Lipkova J, Kofler F, Waldmannstetter D, Delbridge C, Diehl C, Bernhardt D, Schmidt-Graf F, Gempt J, Combs SE, Zimmer C, Menze B and Wiestler B. Towards Image – Based Personalization of Glioblastoma Therapy A Clinical and Biological Validation Study of a Novel, Deep Learning – Driven Tumor Growth Model. Preprint (Version 1) available at Research Square https://doi.org/10.21203/rs.3.rs-2262631/v1
- [2] Ezhov I, Scibilia K, Franitza K, Steinbauer F, Shit S, Zimmer L, Lipkova J, Kofler F, Paetzold JC, Canalini L, Waldmannstetter D, Menten MJ, Metz M, Wiestler B and Menze B. Learn-Morph-Infer: A new way of solving the inverse problem for brain tumor modeling. Med Image Anal. 2023 Jan;83:102672. https://doi.org/10.1016/j.media.2022.102672.
3.15 Conceptual mathematical tumor models on different scales
Barbara Wohlmuth (TU München – Garching, DE)
License: ![]() Creative Commons BY 4.0 International license © Barbara Wohlmuth
Creative Commons BY 4.0 International license © Barbara Wohlmuth
Joint work of: Barbara Wohlmuth, Tobias Duswald, Marvin Fritz, Tobias Köppl, T. Oden, Andreas Wagner
Tumor simulations require complex multiscale models ranging from discrete agent-based models to continuum models, with various hybrid type models in between [1]. Extremely small scales require an agent-based formulation for the tumor and the capillaries, where only signaling molecules, drugs, and nutrients are described by continuous fields [2]. Larger tumors inside rat brains might be resolved with a continuous phase field approach, where still the capillary flow is described by 1D-models, and their growth is modeled by a rule-based algorithm [5]. On the macro scale, the capillaries might be further simplified to a porous medium, requiring only the resolution of larger vessels by 1D-models for breast tumors [7] or 2D surface sources in the lung [8]. Often a problem-dependent coupling is required to achieve a biologically meaningful value range, particularly for the pressure of the 1D blood flow where 0D models have to damp down oscillations.
Besides the choice between discrete and continuum approaches, there remains the question of which biophysical mechanisms are considered relevant for the application at hand and thus have to be modeled, often leading to increasingly complex models of various species. The tumor typically consists of necrotic, hypoxic, and proliferative cell species. For agent-based models, the latter might be further divided into the Q, G1, SG2 subspecies [2]. Further, matrix degenerative enzymes acting on the extra-cellular matrix might be added [3]. The nutrient field might be split up into various porous media resulting in double continuum models [7, 8]. For angiogenesis, vascular endothelial growth factors have to be included [2, 5]. Often mechanical deformations have to be considered [6], and, depending on the clinical therapy, one or more drug species have to be included [6, 8].
All these modeling choices lead to complex, heavily-coupled, nonlinear models, which pose mathematical challenges to the analysis of their well-posedness [3, 4], to the creation of stable numerical schemes and efficient decoupled solvers [5].
In a second, more applied and challenging step, these models have to be calibrated against real-world data [9] and verified against clinical measurements [8]. Here, the amount of data is often the bottleneck and requires a strong multidisciplinary effort to acquire, evaluate and interpret. Especially the derivation of generally accepted benchmark problems for model validation would be extremely valuable for future work.
References
- [1] Lowengrub, John S., et al. “Nonlinear modelling of cancer: bridging the gap between cells and tumours.” Nonlinearity 23.1 (2009): R1.
- [2] Duswald, Tobias, et al. “A Hybrid PDE and Agent Based Model for Cancer Simulations” (preliminary title). in preparation.
- [3] Fritz, Marvin, et al. “Local and nonlocal phase-field models of tumor growth and invasion due to ECM degradation.” Mathematical Models and Methods in Applied Sciences 29.13 (2019): 2433-2468.
- [4] Fritz, Marvin, et al. “Analysis of a new multispecies tumor growth model coupling 3D phase-fields with a 1D vascular network.” Nonlinear Analysis: Real World Applications 61 (2021): 103331.
- [5] Fritz, Marvin, et al. “Modeling and simulation of vascular tumors embedded in evolving capillary networks.” CMAME (2021).
- [6] Fritz, Marvin, et al. “On a subdiffusive tumour growth model with fractional time derivative.” IMA Journal of Applied Mathematics 86.4 (2021): 688-729.
- [7] Fritz, Marvin, et al. “A 1D–0D–3D coupled model for simulating blood flow and transport processes in breast tissue.” IJNMBE (2022).
- [8] Fritz, Marvin, et al. “A phase-field model for non-small cell lung cancer under the effects of immunotherapy.” to be submitted.
- [9] Lima, E. A. B. F., et al. “Calibration of multi-parameter models of avascular tumor growth using time resolved microscopy data.” Scientific reports 8.1 (2018): 14558.
4 Panel discussions
4.1 Working Groups and Panel Discussions
Andreas Mang (University of Houston, US), George Biros (Univ. of Texas at Austin, US), Björn H. Menze (Universität Zürich, CH), and Miriam Schulte (Universität Stuttgart, DE)
License: ![]() Creative Commons BY 4.0 International license © Andreas Mang, George Biros, Björn H. Menze, and Miriam Schulte
Creative Commons BY 4.0 International license © Andreas Mang, George Biros, Björn H. Menze, and Miriam Schulte
As mentioned in the executive summary, the scientific presentations were followed by a brief discussion about selected topics in two working groups to identify immediate goals and further discuss existing challenges. The first group included researchers with a key interest in designing methods to analyze medical (imaging) data and integrate mathematical and computational methods with imaging and medical data. The second group discussed topics associated with the design of mathematical and computational methods for inference, simulation, and optimization. Below we list the key findings in these two groups and some of the questions that remain open.
Working Group 1
We summarize the main topics discussed in the first working group below:
One of the questions discussed during our meeting was if it is possible to curate a database of (publicly) available data for model validation on unseen data in both machine learning and classical modeling. Several questions arose in this context. For example: What are the quality requirements for the data and what datasets are already available? (What are the resolution requirements? How do we deal with medical imaging artifacts?) What are the most pertinent/viable applications that this database is generated from? Do we only include/want longitudinal data included in this study? What types of imaging modalities are most pertinent/relevant and available? Do we require multi-modal/multi-parametric data? What is the best entry-level for these data, i.e., what preprocessing should be applied? How does one coordinate IRB approval across institutions? Another key aspect discussed during this session was the inclusion of meta-data in such a database. Such inclusion is decisive for clinicians and the reproducibility of (modeling and simulation) results. From purely a technological point of view, one needs to decide how to store/curate this metadata in the most efficient way. Moreover, one needs to define a precise protocol to avoid confusion and have documentation. In addition, standards need to be established for data pre-processing. For example, one could improve data sets by offering data correction algorithms to generate a harmonized reference data set and correct for most common imaging artifacts. This would aid reproducibility. Additionally, one could provide data with respect to different processing levels using already available tools deployed by the medical imaging and image computing community.
Another key question that was discussed during this session is how to establish a benchmark and demonstrators for mathematical modeling and data processing. Some of the main questions that arose during this discussion include: What are the representations that models have to return to be useful for clinical evaluation? Can we provide a benchmark that is useful for model development and/or model validation? If so, what are the best metrics for such an effort? How can we quantify tumor or patient status and what are the key metrics most clinicians trust in this context? One possibility is to establish a benchmark similar to the BraTS dataset at the organ level for tumor models. A first step towards establishing such a benchmark could be to develop internal demonstrators to showcase what we can accomplish with available modeling tools to the community at large as well as to clinicians.
Working Group 2
We summarize the main topics discussed in the second working group below:
One of the main challenges for many research groups working in medical imaging sciences is access to clinical data (of high quality). Data is rarely shared amongst groups. One major outcome we hope to accomplish with this seminar is to establish and curate a list of available datasets.
We also discussed aspects surrounding model selection. We discussed the option to drive an initiative for model selection and provide guidance to people with the following aspects in mind: () How do we identify required model complexity with a specific application in mind (i.e., what do the models need to capture in the context of a particular application), () When is a model useful and for what purpose? Can we provide guidance on the usefulness of particular models for specific applications/clinical questions? () What aspects can and should be captured by mathematical models to make them clinically useful? For example, can we include models of radio-necrosis? Are we able to design mathematical modes that can predict pseudo-progression? In this context, we concluded that an attainable concrete goal for participants in this seminar is to curate a list that identifies classes of models and their potential applications. We intend to curate this list in an online platform.
Another key aspect we discussed was model validation and the design of benchmarks for computational models. One challenge in developing benchmarks for mathematical models of disease progression is the definition of a clinical goal and/or a biological phenomenon one wants to capture and how to measure a model’s performance in capturing it. Moreover, we discussed that it will also be instrumental for developing predictive capabilities to rigorously equip our simulations and model-based predictions with certificates about our belief in their accuracy (uncertainty quantification).
Panel Discussion
After the two breakout sessions described above, we came together for a panel discussion. We focussed on the following main items in an attempt to curate some of the information that may help us to push forward community efforts towards developing computational methods to aid clinical decision-making:
As a first attainable goal, we agreed that we would curate a list that identifies individual researchers one reaches out to for computational tools and medical imaging data. Moreover, we discussed how we could support such an endeavor of establishing a clinical benchmark financially, i.e., we identified potential funding agencies to support such an effort. We also identified several long-term goals of key clinical relevance such as differentiation of progression and pseudoprogression (i.e., radio necrosis). Moreover, we established that such a database should provide information about publicly available data sets as well as different classes of models and computational tools for data pre- and post-processing developed by individual groups. We agreed to use GitHub as a starting point to curate a platform to share our research results, methods, algorithms, and data as well as provide a platform for young researchers to showcase their academic profile.
5 Participants
-
Michal Balcerak – Universität Zürich, CH
-
George Biros – Univ. of Texas at Austin, US
-
Sarah Brüningk – ETH Zürich – Basel, CH
-
Malte Brunn – Universität Stuttgart, DE
-
Andreas Deutsch – TU Dresden, DE
-
Matthias J. Ehrhardt – University of Bath, GB
-
Elies Fuster Garcia – Technical University of Valencia, ES
-
David Hormuth – University of Texas at Austin, US
-
Ender Konukoglu – ETH Zürich, CH
-
Jonas Latz – Heriot-Watt University – Edinburgh, GB
-
Guillermo Lorenzo – University of Pavia, IT & UT Austin, US
-
Arvid Lundervold – University of Bergen, NO
-
Andreas Mang – University of Houston, US
-
Björn H. Menze – Universität Zürich, CH
-
Dorit Merhof – Universität Regensburg, DE
-
Daniel Paech – Universitätsklinikum Bonn, DE
-
Sarthak Pati – University of Pennsylvania, US
-
Miriam Schulte – Universität Stuttgart, DE
-
Koen Van Leemput – Martinos Center – Charlestown, US
-
Jonas Weidner – TU München – Klinikum rechts der Isar, DE
-
Benedikt Wiestler – TU München – Klinikum rechts der Isar, DE
-
Barbara Wohlmuth – TU München – Garching, DE
![[Uncaptioned image]](x3.jpg)
6 Remote Participants
-
Atle Bjornerud – University of Oslo, NO
-
Chao Li – University of Cambridge, GB
-
Jana Lipkova – Harvard University – Boston, US
-
Assad Oberai – USC – Los Angeles, US
-
Russell Rockne – City of Hope – Duarte, US