Extended Reality for the Operating Room (XR4OR)
Abstract
This report documents the program and the outcomes of Dagstuhl Seminar 25062 “Extended Reality for the Operating Room (XR4OR)”.
Keywords and phrases:
operating room, scientific roadmapSeminar:
February 2–7, 2025 – https://www.dagstuhl.de/250622012 ACM Subject Classification:
Applied computing Health informatics ; Human-centered computing Virtual realityCopyright and License:
1 Executive Summary
Peter Haddawy (Mahidol University – Salaya, TH)
Anja Hennemuth (Charité – Berlin, DE)
Ron Kikinis (Harvard Medical School – Boston, US)
Gabriel Zachmann (Universität Bremen, DE)
License: ![]() Creative Commons BY 4.0 International license © Peter Haddawy, Anja Hennemuth, Ron Kikinis, and Gabriel Zachmann
Creative Commons BY 4.0 International license © Peter Haddawy, Anja Hennemuth, Ron Kikinis, and Gabriel Zachmann
The first day started with flash talks where participants could introduce themselves and present their work relevant to the Dagstuhl Seminar. In the afternoon, we discussed the overall outcome of the seminar in the group, a potential research roadmap paper, in order to build a common understanding and engagement with the topic. We also showcased about 10 demos, which several participants brought, so that all participants could get an impression of the current state of the art, and also in order to get everybody in the theme of the seminar. This proved to be very successful, even though participants had to bring all the VR hardware themselves.
Tuesday morning was dedicated to introducing the pain points that surgeons face in their daily work in the operating room to the non-medical attendees, i.e., the virtual reality experts and researchers. We had four talks by four surgeons, each one followed by discussions in order to gain a better understanding. The rest of the day was dedicated to generating a large number of ideas, some of which addressed the pain points, but many of them also were generated very creatively by the participants in break-out sessions using the brain-writing method. At the end of the day, participants presented their best ideas in the whole group. After dinner, the organizers sat down together in order to cluster all the ideas and create larger umbrella themes.
On Wednesday, the day began by presenting the clusters to all attendees, and by partitioning the group so that each cluster could be taken care of in break-out sessions. The rest of the day was filled by fleshing out the cluster themes and providing more details with the overarching research themes. On Wednesday night, the organizers sat down to create a framework document, to be used on Thursday for starting the writing process.
Thursday was dedicated to collaborative writing. To do so, each theme was further structured by the attendees, some themes were broken down into smaller sub themes, some of them were already narrow enough, so that in the end, we wrote in pairs on each and every topic.
On Friday, we discussed a number of opportunities and possibilities that would allow us to continue this collaboration as a group. To do so, the organizers presented all the possible funding opportunities we were aware of, and we collected some more from the audience. We also discussed a timeline, in order to produce a research roadmap, and we discussed next steps.
Future activities will include writing and publishing a collaborative paper, where each participant will contribute to one section. The paper is to provide perspectives on trends and future research on the seminar’s topic, and also it can serve as a guideline or roadmap for researchers who like to enter this field. Further activities will strive to establish and broaden a community around the seminar’s topic, by organizing workshops at prestigious VR conferences, such as IEEE VR. Eventually, we will apply for another Dagstuhl Seminar, with a broader participant list, and a somewhat broader topic.
2 Table of Contents
3 Overview of Talks
3.1 Bringing Augmented Reality into the Operating Room: Challenges and Opportunities
Philippe C. Cattin (Universität Basel – Allschwil, CH)
License: ![]() Creative Commons BY 4.0 International license © Philippe C. Cattin
Creative Commons BY 4.0 International license © Philippe C. Cattin
At XR4OR, Philippe C. Cattin presented his research on virtual reality (VR) planning for complex surgical interventions using the Specto Volume Rendering application. He also demonstrated how these planning tools can be transferred into the operating room. While modern surgical loupes reduce eye strain and improve ergonomics during procedures, they also limit the field of view, making it difficult for surgeons to maintain an overview of the entire surgical scene. To address this limitation, integrating augmented reality (AR) into surgical loupes offers a promising solution. AR overlays can provide real-time guidance – such as anatomical landmarks, navigation cues, segmented tumors, or hemodynamic data – without requiring the surgeon to look away from the operative field. By seamlessly blending essential information into the surgeon’s line of sight, AR-enhanced loupes can improve situational awareness, support better decision-making, and ultimately contribute to safer and more efficient surgeries. However, no medically certified AR-enhanced surgical loupes are currently available on the market. This needs to be addressed soon by the MedTech Industry. Despite their potential, deploying VR and AR technologies for routine hospital use remains challenging. Beyond their excellent visual experience, AR/VR systems must prove their clinical effectiveness and efficiency. Medical professionals are only likely to adopt these tools broadly if they demonstrably save time in their already busy schedules. One major barrier is the time-consuming and often unreliable setup process. Connectivity issues with AR/VR glasses, frequent system reboots, and general instability make these solutions impractical for daily clinical use – issues that may be tolerated in research settings, but not in routine care. Another obstacle to clinical integration is the lack of standardized interaction interfaces across different AR/VR hardware manufacturers. While laptops universally rely on keyboards and mice, AR/VR devices use a wide array of input methods. Some manufacturers rely on hand controllers with varying designs and button layouts; others use hand tracking with different gesture sets. These inconsistencies hinder seamless adoption and training, further slowing down the integration of AR/VR into clinical workflows.
3.2 Interactive rendering techniques for mixed reality simulation, planning and guidance of surgical operations
Simon Drouin (ETS – Montreal, CA)
License: ![]() Creative Commons BY 4.0 International license © Simon Drouin
Creative Commons BY 4.0 International license © Simon Drouin
Joint work of: Andrey Titov, Simon Drouin, Alejandro Olivares Hernandez, Tina Nantenaina, Naomi Catwell
This presentation highlighted recent advances by my group on the interactive rendering of medical images for simulation, planning and guidance of surgical operations, with a specific focus on mixed reality displays. We have shown how advanced volumetric rendering techniques can help visualize 4D echography images, how segmented volumes can be interactively volume-rendered in virtual reality to improve depiction of the anatomy for surgical planning and how these interactive rendering techniques can be leveraged to simulate surgical procedures for the training of residents. Following the presentation, a demo of our VR interactive volume rendering system was setup for other seminar participants to try.
3.3 XR Interaction in the Operation Room
Tanja Döring (Universität Bremen, DE)
License: ![]() Creative Commons BY 4.0 International license © Tanja Döring
Creative Commons BY 4.0 International license © Tanja Döring
As a researcher in Human-Computer Interaction, the focus of my work is on innovative and multimodal interaction techniques in different application domains. The domain of the operating room (OR), with its phases of training, preoperative, interoperative, and postoperative activities, offers a multitude of possibilities to be supported by interactive technology to make the procedures more efficient and successful, to improve patient safety and well-being as well as the work conditions of surgeons and OR staff. Nowadays, many digital systems already support the work in the OR, such as by providing image data during surgery. However, the interaction with these systems is often cumbersome, as it takes place as a secondary task next to the primary operation task in sterile conditions and with usually busy hands. Thus, solutions for the interactions with the increasing number of systems are needed that fit this specific and safety-critical environment, align well with the main task of the operation, and do not increase workload. A rise of systems that use extended reality (XR) and artificial intelligence (AI) to provide more extensive assistance to surgeons and medical staff will also set new requirements for the interaction with technology during training, preoperative planning, during surgery in the operating room, and postoperative care. A well-balanced design of embodied, multimodal implicit and explicit XR interactions that also consider a trustful and sensible human-AI collaboration is needed. During the Dagstuhl Seminar “Extended Reality for the Operating Room” we fruitfully discussed this highly interdisciplinary, applied, and dynamic field of research from many angles, compiling visions for smooth, intelligent, and effective XR systems of the future. I am interested in working on a design space for XR interaction in the OR, putting together the dimensions that need to be taken into account when designing for this domain, which include the different phases, tasks and goals, the user roles as well as (explicit and implicit) input and output facilities. Especially the integration of implicit interaction, such as through the tracking of eye gaze and biosensing for input, or the inclusion of additional modalities for output, such as haptic feedback, are promising paths to facilitate and enrich XR interactions in the OR. Nowadays, many parallel systems and screens exist that are not integrated. The usability of used XR systems, such as HMDs, still needs to be improved, and interactions lack standards, so they may be challenging to learn and remember. Thus, there is a great demand for standardization and integration and the design of personalized and context-aware, more intelligent interactive assistance systems.
3.4 Gabor Fichtinger: directions for future grants
Gabor Fichtinger (Queen’s University – Kingston, CA)
License: ![]() Creative Commons BY 4.0 International license © Gabor Fichtinger
Creative Commons BY 4.0 International license © Gabor Fichtinger
During the Dagstuhl Seminar, I focused on developing research project ideas and exploring directions for future grant proposals. I also contributed to drafting a joint white paper that brought together perspectives from different participants to outline shared research priorities. In addition, I met several researchers whose work intersects with mine, leading to new academic connections that may support future collaboration. The seminar provided time and space for thoughtful exchange, helping identify common interests and potential pathways for joint work in global health.
3.5 Imaging data and preoperative planning as main components for XR in the operating room
Tabea Flügge (Charité – Berlin, DE)
License: ![]() Creative Commons BY 4.0 International license © Tabea Flügge
Creative Commons BY 4.0 International license © Tabea Flügge
Extended Reality in the operating room may enhance surgical precision, efficiency, and patient outcomes. Key aspects are the accurate registration and display of multimodal imaging data and the transfer of the preoperative planning to the surgical site. XR may provide real-time 3D overlays of patient anatomy, helping surgeons navigate complex procedures with greater accuracy. The holographic visualization of critical structures, like blood vessels, tumors, or nerves, may reduce surgical risks. Transferring preoperative planning to the surgical site allows for real-time navigation of procedures. The surgeon receives intraoperative guidance by superimposing 3D images of the planned surgical result on the region of interest. In reconstructive oral and maxillofacial surgery cases, complex preoperative planning is performed, and surgical guides and patient-individual implants are manufactured. Therefore, adherence to the surgical plan is crucial for avoiding intra- and postoperative complications. Incorporating automated segmentation and analysis of large amounts of patient data further helps predict surgical risks and machine learning models may suggest surgical approaches to improve the precision of a surgical procedure. A second key aspect besides the availability of information is its individual display, e.g., on head-mounted devices, to avoid distraction and work continuously without breaking focus. User profiles for all staff members in the OR may improve the distribution of information in the OR and avoid redundant information.
3.6 LARACROFT: A Collaborative AR Platform for Enhancing Laparoscopic Training in the Operating Theater
Joaquim A. Jorge (University of Lisbon, PT)
License: ![]() Creative Commons BY 4.0 International license © Joaquim A. Jorge
Creative Commons BY 4.0 International license © Joaquim A. Jorge
Joint work of: Joaquim A. Jorge, António Salgueiro, Mona Zavichi, Anderson Maciel, Catarina Moreira, Francisca Leite, Cátia Costa
The LARACROFT platform introduces an augmented reality (AR) framework tailored for remote collaboration in laparoscopic surgery. Designed to operate within the spatial and cognitive constraints of the operating theater, the system supports real-time interaction between local and remote surgeons via a shared AR workspace. It integrates hand tracking, video passthrough, and gaze-directed, foot-triggered input mechanisms to enable effective control without compromising sterility or workflow. In a pilot study, medical students and mentors engaged in standardized surgical tasks, revealing key insights into the impact of AR-supported telecollaboration on motor coordination and communication. Observed limitations, including latency and display resolution, highlighted current technological thresholds in surgical AR. However, participants reported enhanced engagement and situational awareness, pointing toward the platform’s potential for scalable deployment in surgical education and support.
3.7 Workflow Considerations for XR in the OR
Luv Kohli (InnerOptic Technology – Hillsborough, US)
License: ![]() Creative Commons BY 4.0 International license © Luv Kohli
Creative Commons BY 4.0 International license © Luv Kohli
XR has the potential to be used in a variety of ways for the OR, such as medical device navigation, visualization of internal structures, identification of cancerous tissue, pre-procedure or intra-procedure planning, information and image display, telemedicine and communication, and many more. Rather than focus here on a specific use case, I offer some thoughts and questions about how we might enable XR’s eventual adoption and use in the OR.
There are cases where XR use by patients shows a lot of promise and success (for example, pain distraction, neurological rehabilitation, PTSD). XR technology has advanced considerably in recent years but to my knowledge, it does not yet have widespread adoption in the OR, at least not for physician users. Why?
When researching, developing, and commercializing new technologies for the OR, we face the challenge of how to integrate those technologies into physician workflows. If a new technology takes too much time to set up for each patient, it becomes an opportunity cost with less time available to treat additional patients. If using the technology is too complex, it ends up not being used. For example, some physicians have told me that even though they have access to some sophisticated medical device navigation systems, setup takes long enough that it is not worth the time or complexity.
Also, for an organization to invest in a technology commercialization effort, there must be reasonable evidence that the technology (compared to standard of care or other less disruptive technologies) will improve patient outcomes, enable physicians to do things they otherwise could not do, improve hospital throughput, generate profit for the hospital, or provide some other business benefit.
As researchers and technologists focused on improving patient care with XR, how might we develop XR to enable its use without workflow disruption? For example, what can be done to make setup quick and efficient? How can technology be made robust to failure or emergency situations (e.g., if an emergency arises, can the physician immediately remove a headset and revert to standard of care?)? How can ergonomics be improved, especially for long procedures?
These considerations often end up being procedure-specific because different procedures have different workflow requirements. For complex procedures, a lot of time and mental effort can be spent on communication between physicians and OR staff, so that physicians can see what they need to see. One could imagine developing procedure-specific conversational AI models for a physician to more easily interact via voice, without requiring very precise wording, or without requiring challenging hand gestures or controllers. Procedure-specific inference models may also be able to understand procedure workflow and show “just-in-time” information to the physician, reducing communication overhead.
There are likely many other workflow-related improvements that can be made, and it would be interesting to explore how our research can support physicians and staff in the OR without negatively impacting their workflow.
3.8 Perspective on the Future Use of XR for OR
Mario Lorenz (TU Chemnitz, DE)
License: ![]() Creative Commons BY 4.0 International license © Mario Lorenz
Creative Commons BY 4.0 International license © Mario Lorenz
XR, in a strict sense, only encompasses the mediation of virtual, computer-generated content for all human senses i.e., visual overlays, haptic or acoustic amplifications. However, XR alone is just one of several technologies (AI, image processing, 3D-printing, diagnostics) driving the progress in medicine and surgery and a focus solely on XR without including those other domains will rather hinder than facilitate XRs uptake in the OR. In general, it is important not to ask ourselves “What can XR do for the surgeon?”, but rather “What problems does the surgeons currently have? Where are the limitations of how they can help the patient?” Using this approach, we will discover where XR really brings a benefit and is not just pushed from a technology enthusiastic perspective. We will further discover how XR fits best in to the supporting ecosystem of advanced technologies (AI, image processing, 3D-printing, diagnostics). By facilitating synergies, and win-win-situations, we will foster the transfer into the OR. The following use case shall demonstrate my perspective:
-
1.
Patient with Face/Head-Trauma. When the patient arrives in OR the surgeon could get an overlay of the MRI on the patient using AR. This is not a very new use case, but everything one could achieve solely with XR. By broadening the scope of involved technologies, a much more advanced scenario is imaginable. By 3D-scanning the patients head in the OR an AI could calculate how the bone fragments have moved since the MRI was taken and can visualize this updated 3D-model to the surgeon via an AR headset. Another AI, could deduce how the bone fragments have to be put together stepwise, which implants are necessary for this, how standard implants have to be bend and what custom implants need to be 3D-printed. Once this is determined 3 paralyzed processes are imitated (1) the printing of the custom implants; (2) A nurse or a resident surgeon is adapting the shape of the standard implant using a template of the target shape visualized through and AR display. An AI checks in the background the forming process and provides and audio-visual feedback when the correct shape is reached; (3) The surgeon gets support through the AR glasses by visualising the positions of the bone fragments and the instructions of how they have to be put together using the implants. During the entire surgery the visual guidance is updated based on the tracked deformation of the patient’s soft tissue. Another option for this use case for severe trauma or in case of tumour resection is, that the AI calculating the reconstructions steps also uses pictures form the patient before the incident.
-
2.
Tracking for AR guidance, VR training and automated surgery. In the future OR, every step of the surgery is tracked. This data can be used to generate training scenarios in VR simulation but also to teach an AI to perform surgery autonomously. Further, it allows to gather the various existing individual surgical techniques and may allow to find the objectively best procedures. In AR supported surgical guidance applications this knowledge is used for generating the AR instructions.
-
3.
XR for Telesurgery. In the future telesurgery will not be performed by the surgeon looking at mono- or stereoscopic images of a live feed. Instead, a detailed and complete 3D representation of the patenting will be simulated visually, haptically, auditory and olfactory. This allows the surgeons to perform the surgery on a virtual patient whilst their movements are tracked and translated to according movements of the surgery robot.
-
4.
Miscellaneous Use Cases. (1) AI based detection of a sudden vessel rupture, with AR visualization of the rupture spot. (2) AI based in-situ detection of tumours with AR visualisation and guidance. (3) Integrating of health monitor data and other patient data into a single cockpit that is visualized in AR for the surgeon during surgery.
3.9 Experimenting with augmented reality in the operating room: lessons learned
Javier Pascau (Carlos III University of Madrid, ES)
License: ![]() Creative Commons BY 4.0 International license © Javier Pascau
Creative Commons BY 4.0 International license © Javier Pascau
Joint work of: Javier Pascau, Mónica García-Sevilla, David García-Mato, Rafael Moreta-Martínez, Alicia Pose-Díez-de-la-Lastra
In this talk, I presented our experience at Universidad Carlos III de Madrid introducing Augmented Reality (AR) in the Operating Room (OR). Our initial open-source solution combined a 3D-printed reference, a surgical guide, and an application running on a smartphone, offering a versatile approach for visualizing anatomical models augmented over 3D-printed phantoms or directly onto patients during surgery. With this straightforward method, we successfully displayed essential surgical planning information in training sessions for sacral neurostimulation and during craniosynostosis and microtia surgeries. Smartphones and tablets offer numerous advantages, such as affordability, ease of introduction into sterile environments via transparent bags, and the possibility of sharing the AR visualization among multiple users. However, when porting our AR solutions to Head-Mounted Displays (HMDs) like Microsoft Hololens2, the interaction with holograms and the immersive experience greatly improved. Despite current HMD limitations, this approach offers significant benefits for the OR, including natural hand-gesture interactions and enhanced 3D perception. Our recent work integrating Hololens2 with the 3DSlicer platform has opened new possibilities, combining the advantages of AR visualization with the computational and algorithmic capabilities available in 3DSlicer. These findings were demonstrated after the talk, utilizing a 3D-printed craniosynostosis patient model to visualize AR content both on a tablet and via Hololens2.
3.10 Personal perspective of seminar outcome
Dirk Reiners (University of Central Florida – Orlando, US)
License: ![]() Creative Commons BY 4.0 International license © Dirk Reiners
Creative Commons BY 4.0 International license © Dirk Reiners
The main outcome for me for this seminar is a much better understanding of the needs of the medical professionals in the OR, in terms of things they can and cannot do, and their requirements of supporting technology like XR. Discussions with doctors and XR researchers led to new ideas for visual representations of relevant data in an integrated context that can be used inside the OR for different kinds of procedures.
3.11 Multimodal Features and User Representation Considerations
Anke V. Reinschluessel (Universität Konstanz, DE)
License: ![]() Creative Commons BY 4.0 International license © Anke V. Reinschluessel
Creative Commons BY 4.0 International license © Anke V. Reinschluessel
Several aspects are important to consider in order to advance the use of extended (XR) or mixed reality (MR) in the operating room (OR). When thinking about MR, we mostly focus on the visual aspects, but MR can also augment or integrate other senses, such as audio or haptic, which can also support a procedure. There have been approaches to use audio or tactile information to guide interventions (e.g., [3] or [5]). Furthermore, also for surgery planning, haptic props have been shown as a promising approach to interacting with image data (e.g., [1, 2] or [4]). Multimodal feedback might also be particularly interesting in a situation where a specialist is joining remotely and is virtually present in the room. Subtle on-site occurrences, like a sound from a device or someone coming into the OR asking a question, might not be picked up and transmitted by the collaboration system by default but distract the team on-site. This could lead to confusion as the reason for the team’s attention shift is unclear to the remote specialist. Therefore, it is important to consider what and how it is transmitted in these remote collaboration settings. To create a better sense of co-presence, a system should also not simply represent the position the remote person placed themselves but maybe also add multimodal feedback for the on-site personnel, e.g., heat patches imitating the body heat someone standing there would radiate. Likewise, it might be worthwhile to explore which kind of user representations support remote collaboration best, as humans pick up subtle cues without conscious processing that influence the relationships. For example, our breathing and heart rate are perceived and can synchronise, leading to a feeling of closeness and allowing for an understanding of the other person’s state in real settings, which are details that current avatar representations omit. Additionally, as avatar representations can also be a source of distraction, investigating which aspects of the user representation are beneficial for use in a high-stress environment and which add stress. The aspects of this talk were intensely discussed in the context of remote collaboration for surgical contexts, but might also play a role in robotics-assisted surgery or remote robotic surgery. It is worthwhile to investigate how the humans operating them can be present in the OR, and, potentially, the results can also be transferred to robotics representations to increase awareness and collaboration with it.
References
- [1] Reinschluessel, A., Fischer, R., Schumann, C., Uslar, V., Muender, T., Katzky, U., Kißner, H., Kraft, V., Lampe, M., Lück, T. & Others Introducing virtual & 3D-printed models for improved collaboration in surgery. Proceedings Of The 18. Annual Meeting Of The German Society Of Computer-and Robot-Assisted Surgery, Oliver Burgert (Ed.). 18 pp. 253-258 (2019)
- [2] Reinschluessel, A., Muender, T., Salzmann, D., Döring, T., Malaka, R. & Weyhe, D. Virtual Reality for Surgical Planning – Evaluation Based on Two Liver Tumor Resections. Frontiers In Surgery. 9 (2022)
- [3] Black, D., Lilge, S., Fellmann, C., Reinschluessel, A., Kreuer, L., Nabavi, A., Hahn, H., Kikinis, R. & Burgner-Kahrs, J. Auditory Display for Telerobotic Transnasal Surgery Using a Continuum Robot. J. Medical Robotics Res.. 4, 1950004:1-1950004:14 (2019)
- [4] Muender, T., Reinschluessel, A., Salzmann, D., Lück, T., Schenk, A., Weyhe, D., Döring, T. & Malaka, R. Evaluating Soft Organ-Shaped Tangibles for Medical Virtual Reality. CHI ’22, New Orleans, LA, USA, 29 April 2022 – 5 May 2022, Extended Abstracts. pp. 237:1-237:8 (2022)
- [5] Reinschluessel, A., Cebulla, S., Herrlich, M., Döring, T. & Malaka, R. Vibro-Band: Supporting Needle Placement for Physicians with Vibrations. Extended Abstracts Of CHI 2018, Montreal, QC, Canada, April 21-26, 2018. (2018)
3.12 Enhancing Liver Surgery and Hepatic Interventions with AI and XR Technologies
Andrea Schenk (Fraunhofer MEVIS – Bremen, DE)
License: ![]() Creative Commons BY 4.0 International license © Andrea Schenk
Creative Commons BY 4.0 International license © Andrea Schenk
Artificial intelligence technologies, particularly deep learning, have accelerated and partially automated the analysis of preoperative imaging data such as CT and MRI. This has enabled more widespread creation and use of 3D models for treatment planning, risk analysis and decision support. In particular, liver cancer treatments with multiple therapy options, including open and minimally invasive surgery, have benefited from this development. The addition of information from laboratory values, histology and liver function tests, together with numerical simulations and AI-based prediction of treatment outcomes, has led to simpler, safer and improved therapies. XR tools, particularly augmented reality (AR), provide surgeons with real-time visualizations of complex liver anatomy, enabling greater accuracy during procedures. This enhanced visualization helps to accurately identify critical structures such as blood vessels, bile ducts and distances to tumors, ultimately reducing the risk of complications. The use of XR in surgical training also improves the skills of medical professionals by allowing them to practice techniques in an immersive, risk-free environment. The combination of AI and XR technologies helps ensure that patients receive safer and more effective care in the field of liver surgery, with the potential to significantly improve patient outcomes. In the talk, I presented our own research in this area, including the segmentation of anatomical liver structures and pathologies from CT and MRI data using AI, the calculation of image-based liver function, and therapy simulations for tumor resection and ablation as well as for liver transplantation. In three projects, we extended XR technologies for the transfer of 3D models and planning results into the operating room and developed an extremely fast visualization technology called AVIS, which allows noise-free real-time volume rendering in AR with interactive modification of the transfer function and application of cut planes. An overview of current research topics concluded the presentation.
3.13 Towards task specific (physical) XR solutions
Falko Schmid (Heinrich-Heine-Universitätsklinikum Düsseldorf, DE)
License: ![]() Creative Commons BY 4.0 International license © Falko Schmid
Creative Commons BY 4.0 International license © Falko Schmid
XR is emerging as a valuable tool in the operating room (OR), with the potential to support a range of critical processes and workflows, including immersive communication, visualization of medical imagery, navigation, and ambient communication through technologies such as light and projection. These applications can greatly enhance the effectiveness and efficiency of medical procedures, but to unlock their full potential, several key factors must be addressed. A thorough understanding of the technology itself is essential. Devices like headsets must be carefully evaluated for factors such as battery life, resolution, camera position, field of view, brightness, and sensory capabilities, as these elements significantly impact the quality and feasibility of potential solutions. Additionally, interaction capabilities like gestures, voice control, eye tracking, contextual sensor fusion, and the integration of wearables must be explored to ensure they align with the specific needs of the medical environment. Equally important is a deep understanding of the task at hand. It is crucial to determine whether additional visual information would be beneficial and to evaluate alternative ways to present information, such as through sound, ambient changes, vibration, or external visual cues. It’s not just about identifying the type of information required but also understanding how and when it should be delivered to maximize its value. The implementation of natural, intuitive, and robust interactions is key, especially in high-pressure environments like surgery, where ease of use and minimizing distractions are critical. Finally, a comprehensive understanding of clinical processes is necessary to integrate MR effectively into existing workflows. Solutions must be designed to enhance the capabilities of medical professionals without adding complexity or burden. Given the fragility of MR technology, developing stable, robust, and turnkey solutions that are reliable is a significant challenge that must be addressed to fully realize MR’s potential in the OR. I believe that rethinking what XR means in concrete implementations is necessary. For example, while relying on multi-purpose headsets like HL offers the potential for fast, low-effort showcasing, these devices are often over-engineered, but typically leading to fragile solutions. Too often, our thinking is driven by the technological possibilities of these devices, rather than analyzing the needs of surgeons and the underlying processes. I believe specific solutions, especially in terms of hardware, can be much more beneficial by addressing the real needs of surgeons. For instance, using their native tool – the surgical magnification loupe – as an interface for augmented reality, rather than introducing an entirely new device, could provide a more effective solution.
3.14 XR and AI as collaborative tools for shared decision-making
Siriwan Suebnukarn (Thammasat University – Pathum Thani, TH)
License: ![]() Creative Commons BY 4.0 International license © Siriwan Suebnukarn
Creative Commons BY 4.0 International license © Siriwan Suebnukarn
XR and AI as collaborative tools for shared decision-making XR enhanced by AI has tremendous potential in shared decision-making (SDM) both preoperative and intraoperative surgical contexts by providing data-driven insights, automating routine tasks, and offering predictive analytics to support clinicians in making informed decisions. Using XR, surgeons can interact with anatomical models in a virtual environment, simulating different surgical approaches, testing possible complications, and adjusting the plan in a shared decision-making context. AI can also suggest the most efficient path based on patient-specific factors. AI can process large datasets from similar cases to predict potential risks (e.g., bleeding, infection, recovery time) for a given patient. During shared decision-making, these risk assessments can be integrated into XR, allowing the surgical team to visualize how different decisions (such as incision placement, resection margins) might impact patient outcomes in real-time. In cases where multiple specialists must collaborate on a complex procedure, XR can help them rehearse the surgery together by simulating potential complications or variations, and specialists can practice responding to these challenges in an immersive XR environment before surgery. Preoperative SDM often involves consultations with patients and families. AI-driven XR systems can present the patient’s condition and potential surgical options in an easily understandable format, improving communication and helping the patient become an active participant in the decision-making process. The intraoperative phase is highly dynamic, requiring real-time decision-making based on changing conditions. During surgery, AI can process real-time imaging data (such as live CT, MRI, or ultrasound) and use XR to overlay crucial information onto the surgical field. This allows the surgical team to make shared decisions without losing focus on the procedure. AI can highlight critical structures or suggest optimal surgical paths, reducing the risk of errors. AI can provide real-time decision support by analyzing the evolving intraoperative environment and suggesting changes to the surgical plan. For example, if unexpected bleeding occurs or tissue appears different from preoperative images, AI can process these changes and recommend adjustments, which are then visualized in XR. Surgeons and other specialists can review these suggestions and decide collaboratively on the next steps. By merging the analytical power of AI with the immersive capabilities of XR, teams can enhance collaboration, precision, and patient outcomes in both preoperative planning and intraoperative execution.
3.15 Virtual and Augmented Reality in a Surgical Setting – Research at the University Clinic for Visceral Surgery, Pius-Hospital Oldenburg
Verena Uslar (Universität Oldenburg, DE)
License: ![]() Creative Commons BY 4.0 International license © Verena Uslar
Creative Commons BY 4.0 International license © Verena Uslar
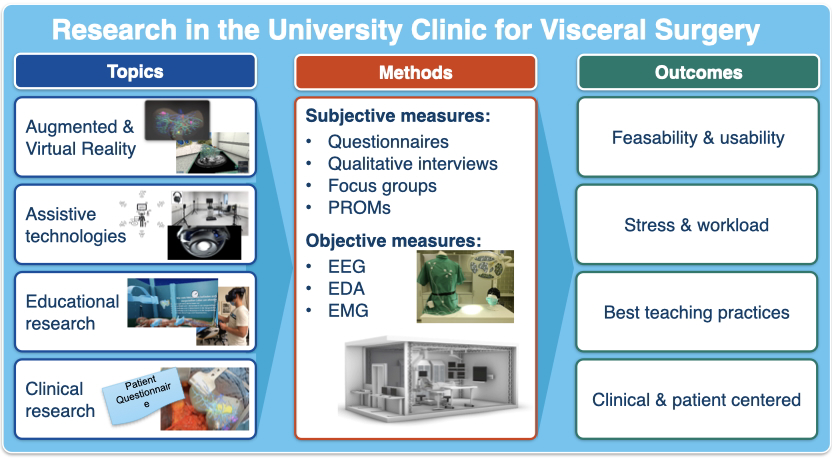
To compensate for the growing personnel shortage in medicine, the possibilities of digitalization must be fully exploited. However, significant problems still exist in transferring new digital tools into clinical practice. Often, medical staff are skeptical about introducing new tools into daily clinical routine and/or the tools do not meet the actual needs. Therefore, the University Hospital for Visceral Surgery at Pius-Hospital, with its research focus, is dedicated to the user-centered development of digital tools in collaboration with developers and companies from the medical technology industry. This ensures that the tools are developed in a needs-based manner from the outset and increases the likelihood of the tools developed in research projects being transferred to a marketable medical product. At the Dagstuhl Seminar XR4OR, I was pleased to have the opportunity to present three best-practice projects and their results. In the VIVATOP project, we researched VR and AR applications for preoperative planning, intraoperative support, and training and further education with our project partners. For example, a VR planning tool was developed that uses a haptically correct liver model instead of conventional controllers for interaction (see Fig. 1). Additionally, an AR application was researched that allows users to view segmented, patient-specific 3D liver models and can also be used intraoperatively as a navigation aid for tumor resection. The follow-up project AHrEZ is currently working on the automatic segmentation of the liver model based on patients’ CT or MRI scans and the automatic placement of the model in the surgical site during the operation.
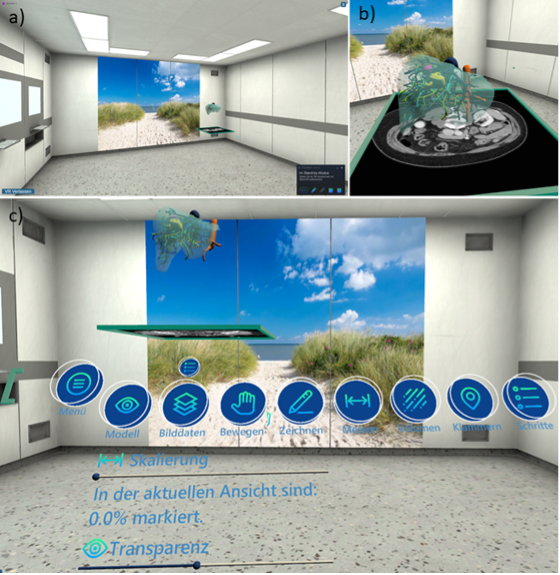
For the evaluation of these tools, the University Hospital for Visceral Surgery uses not only the usual subjective measures known from user-centered development, such as questionnaires or interviews, but also new methods like mobile EEG or skin conductance (EDA). Furthermore, the University Hospital operates two Living Labs, where the developed tools can be iteratively tested (see Fig. 2). This allows us to provide our development partners with a comprehensive overview of factors such as feasibility and usability of the developed tools, as well as workload and stress when using the tools, in research projects. This leads to demonstrators, such as the newly developed lighting concept for the operating room in the SmartOT project (see Fig. 3), being researched in a sustainable manner, so that the implementation as a medical product actually occurs after the project.

The Dagstuhl Seminar was a confirmation for me that this type of research is urgently needed. Additionally, it had a lasting impact on future research projects through the creation of new contacts.
3.16 Awake Craniotomy
Gregory F. Welch (University of Central Florida – Orlando, US)
License: ![]() Creative Commons BY 4.0 International license © Gregory F. Welch
Creative Commons BY 4.0 International license © Gregory F. Welch
The following is an idea I wrote up to share, but then discovered that it is already being done, at least to some extent. Still, I like the idea, and think more could be done in this area.
Awake neurosurgery , also known as awake craniotomy , is a specialized surgical procedure performed while the patient is conscious. This technique is often used when operating on brain regions responsible for critical functions like language, motor control, and memory, to monitor and preserve the patient’s cognitive and functional abilities in real-time.
Although I am not a medical professional, I have seen this in person. My mother suffers from Essential Tremor (ET) – a neurological disorder that causes involuntary, rhythmic shaking, typically affecting the hands but sometimes impacting other parts of the body, such as the head, voice, arms, or legs. I was present in the operating room when she had a Deep Brain Stimulation (DBS) system implanted for the first time, and again when she had revision surgery – surgical repositioning of the leads / contacts in her brain.
My thinking is that an awake neurosurgery patient could wear a VR system running an application that automatically, with the guidance of the surgeon, prompts the patient to think and speak about things, perhaps even to carry out cognitive and motor activities. The goal would be to exercise different regions of the brain during the surgery, to increase the chance of detecting any neurological issues caused by the surgery.
For example, much like VR is used for physical therapy, the system could present the patient with nearby virtual targets to look at or even “touch”. This could be going on concurrently while the surgeon is operating, normally cycling through some critical activities (cognitive functions), and / or carrying out activities that exercise parts of the brain called out by the surgeon. While the surgeon could call out the specific activities, if they instead call out the goal for the cognitive activity, the system could undertake a broad series of activities that will stimulate or exercise the relevant brain activity.
3.17 Haptics for the OR
Rene Weller (Universität Bremen, DE)
License: ![]() Creative Commons BY 4.0 International license © Rene Weller
Creative Commons BY 4.0 International license © Rene Weller
Joint work of: Rene Weller, Gabriel Zachmann, Maximilian Kaluschke, Siriwan Suebnukarn, Peter Haddawy
Haptic feedback plays a crucial role in realistic surgical simulation and has the potential to enhance actual surgical procedures. We will detail the development of a VR simulator for total hip arthroplasty (THA) and dental surgeries, including the haptic devices, rendering methods, and evaluation of its realism and usability. Furthermore, we discuss how haptic interfaces and devices can be applied in the operating room, focusing on how providing tactile feedback to surgeons can improve precision, safety, and control, ultimately leading to better surgical outcomes.
3.18 Remotely guided robotic surgery through extended reality
Sudanthi Wijewickrema (University of Melbourne, AU)
License: ![]() Creative Commons BY 4.0 International license © Sudanthi Wijewickrema
Creative Commons BY 4.0 International license © Sudanthi Wijewickrema
In locations where expert surgeons are not available, it will be beneficial if remote surgery is possible. This will require the following.
Obtain a model of the region of interest: Pre-operative scans of the patient (regions of interest for the surgery) need to be obtained first. These scans should then be segmented to identify anatomical structures and/or pathologies. Artificial intelligence methods such as deep learning can be used for this. From these segmentations, a 3D model of the region of interest can be created.
Generate a surgical plan: Using the pre-operative 3D model, a surgical plan and optimal path for the surgery should be generated. The path should be displayed on the 3D model in a step-by-step manner to enable real-time guidance.
Register the patient with the pre-operative model: Fiducials can be used as orientation landmarks to register the patient with the 3D model and surgical plan. Registration should be done prior to the start of the surgery and in real-time to ensure the 3D model is aligned with the patient.
Perform remote robotic surgery: The surgeon in the remote location can operate on the 3D model projected via a XR headset and haptics that simulate the robotic surgical system. The operation will be reflected on the actual patient mimicking the actions of the remote surgeon.
4 Open problems
4.1 Dagstuhl Seminar 2025 – XR in the OR: “Pain Points”
Dirk Weyhe (Universität Oldenburg, DE)
License: ![]() Creative Commons BY 4.0 International license © Dirk Weyhe
Creative Commons BY 4.0 International license © Dirk Weyhe
Main reference: Weyhe D. (2025): Neue digitale Assistenzsysteme: Potenziale in der Viszeralmedizin. Die Chirurgie. 96, 1-2. doi: 10.1007/s00104-024-02220-9
Introduction.
The future of medicine in the Western world is shaped by demographic change and increasingly advanced, individualized, and interdisciplinary therapy options. In contrast, there is a growing shortage of personnel. The Wi-FOR Institute, commissioned by Price Waterhouse Coopers (PWC) Germany, analyzed that in 2022, there was a shortage of 290,000 unfilled positions (6.8%) in the healthcare sector, which is expected to grow to 1.8 million (35.4%) by the year 2035. The Robert Bosch Foundation published a study in 2021 titled “Health Centers for Germany: How a Restart in Primary Care Can Succeed.” Their projections indicate that by 2035, rural areas, such as Northwest Germany, will face dramatic undersupply with a primary care coverage rate of less than 75%. The German Medical Association describes in the report on “Resilience in Healthcare” from 2023 by the Expert Council that the increasing demand for medical expertise will be met with a future shortage of doctors.
Method.
The potentials of digital assistance systems such as AR and VR are presented using the example of the BMBF-funded collaborative project VIVATOP (Weyhe, 2025). In this project, preoperative liver surgeries were planned in VR based on patient-specific segmented DICOM data (CT scans), supported intraoperatively by AR, and the case series was transferred into a database for postoperative debriefing and training purposes. Initial combinations of 3D-printed livers and registered AR projections for training purposes are presented (Fig. 4).

As “pain points” for potential routine application, “Fluid XR in daily use”, “automatic placement” (registration), fully automatic segmentation (3D), “haptic feedback” in planning & training systems, and very important digital concepts to compensate for the lack of healthcare workers have been defined.
Summary
The potential of digital assistance systems in visceral surgery is enormous; however, a number of technical solutions are still needed to fully realize these potentials in routine practice with high added value. In this context, telemedicine plays a crucial role and has made significant advancements in recent years.
References
- [1] Dirk Weyhe. Neue digitale Assistenzsysteme: Potenziale in der Viszeralmedizin. Die Chirurgie. 96, 1-2. doi: 10.1007/s00104-024-02220-9
5 Participants
-
Philippe C. Cattin – Universität Basel – Allschwil, CH
-
Tanja Döring – Universität Bremen, DE
-
Simon Drouin – ETS – Montreal, CA
-
Gabor Fichtinger – Queen’s University – Kingston, CA
-
Tabea Flügge – Charité – Berlin, DE
-
Peter Haddawy – Mahidol University – Salaya, TH
-
Anja Hennemuth – Charité – Berlin, DE
-
Joaquim A. Jorge – University of Lisbon, PT
-
Ron Kikinis – Harvard Medical School – Boston, US
-
Luv Kohli – InnerOptic Technology – Hillsborough, US
-
Mario Lorenz – TU Chemnitz, DE
-
Rainer Malaka – Universität Bremen, DE
-
Javier Pascau – Carlos III University of Madrid, ES
-
Dirk Reiners – University of Central Florida – Orlando, US
-
Anke Reinschlüssel – Universität Konstanz, DE
-
Andrea Schenk – Fraunhofer MEVIS – Bremen, DE
-
Falko Schmid – Heinrich-Heine-Universitätsklinikum Düsseldorf, DE
-
Siriwan Suebnukarn – Thammasat University – Pathum Thani, TH
-
Verena Uslar – Universität Oldenburg, DE
-
Gregory F. Welch – University of Central Florida – Orlando, US
-
Rene Weller – Universität Bremen, DE
-
Dirk Weyhe – Universität Oldenburg, DE
-
Sudanthi Wijewickrema – University of Melbourne, AU
-
Gabriel Zachmann – Universität Bremen, DE
![[Uncaptioned image]](x3.jpg)